Status mundi in tempore coronavirus
Fututi sumus atque nec ignoramus. I mean, we’re fucked up, and we very well know it, but is it there still hope? I’m struggling to find the light at the end of the COVID-19 tunnel, and I’m not sure that there is one.

As much as I said I cannot stand it and I won’t write about COVID-19 anymore, what’s left to life is not COVID-19? Well, some more facts and thoughts, then.
Non-COVID-related first
While it’s too early to get post-COVID PTSD, because the COVID-19 crisis is still ongoing, it’s not too early to get depressed owing to other news that attest the world’s suicidal idiocy.
How about the Volkswagen no longer making cars with internal combustion engines in Europe by 2035, in accordance to EU’s “Greta Thunberg” policy? (Since 2036, the only new cars purchasable in the EU will be fully electric. I suppose that’s the day when Europe will be officially dead.) How about Daimler (Mercedes-Benz) saying that all their new vehicle platforms will only make EVs from 2025? (And this helped their shares raise by 2.5%!)
And what is to be understood of the “digital euro” (terrible misnomer, as all money are already digital, and they stay this way unless you want to cash physical banknotes) the European Central Bank insist they want to launch? There are actually many other central banks experimenting with CBDC (Central Bank Digital Currency)! The official ECB explanation is useless, as they only say the “digital euro” won’t replace, but only complement the regular euros that can be cashed. Reuters says that the amount of “digital euros” an individual can own would most likely limited at w.g. €3,000, or higher amounts might be penalized, which makes the entire project seem even more futile? What are those fucktards doing with our lives, why are they trying to destroy the human civilization?!
N26 comes with a better analysis. Apparently, this is ECB’s attempt to counter the cryptocurrencies. The “digital euros” will use the blockchain technology, but they’ll be backed by the ECB. No other bank will be involved, and no bank account is needed, but a digital wallet must be created, and the money can be deposited directly with the ECB! Why don’t they do the other way around, then, i.e. to let people deposit their “normal money” with the ECB and let the commercial banks only give loans with digital currency?
The advantages of the “digital euro” are still only some words which, when you read them, make no sense. Not much more than Stalin’s and Ceaușescu’s speeches, anyway.
Back to more tangible (and less fungible) stuff, while Intel wants to invest $20bn in chip factories in the EU (Taiwan’s TSMC too is eyeing Europe!), some analysts consider Europe’s enthusiasm to be wrong: first, because 90 percent of European chip needs until the end of this decade will be for chips of above 10 nm (we need the cheap stuff, right?), and secondly, “the EU is wrong to focus on manufacturing rather than on chip design, which is the part of the production process with the highest value added.” Basically, the fucktards use the same approach that deindustrialized Europe, this time being keen to replace the dependence of China with the dependence of no matter what other country or countries! On the other hand, it’s true that “we should worry about who designs them — because it’s definitely not us,” and that “having a factory in your back garden” doesn’t necessarily fix the supply chain risk. We’re too deep in this shit, and too reliant on all kind of parts and materials coming from everywhere else! (Heck, from the 1960s-1970s through the early 1990s, even the Communist countries in Europe were making semiconductors and all kinds or electronic components!)
There are also plans to invest €40bn in 38 factories that would manufacture car batteries in Europe, but this “will not enable [Europe] to meet anywhere close to all of its internal demand for EV batteries.”
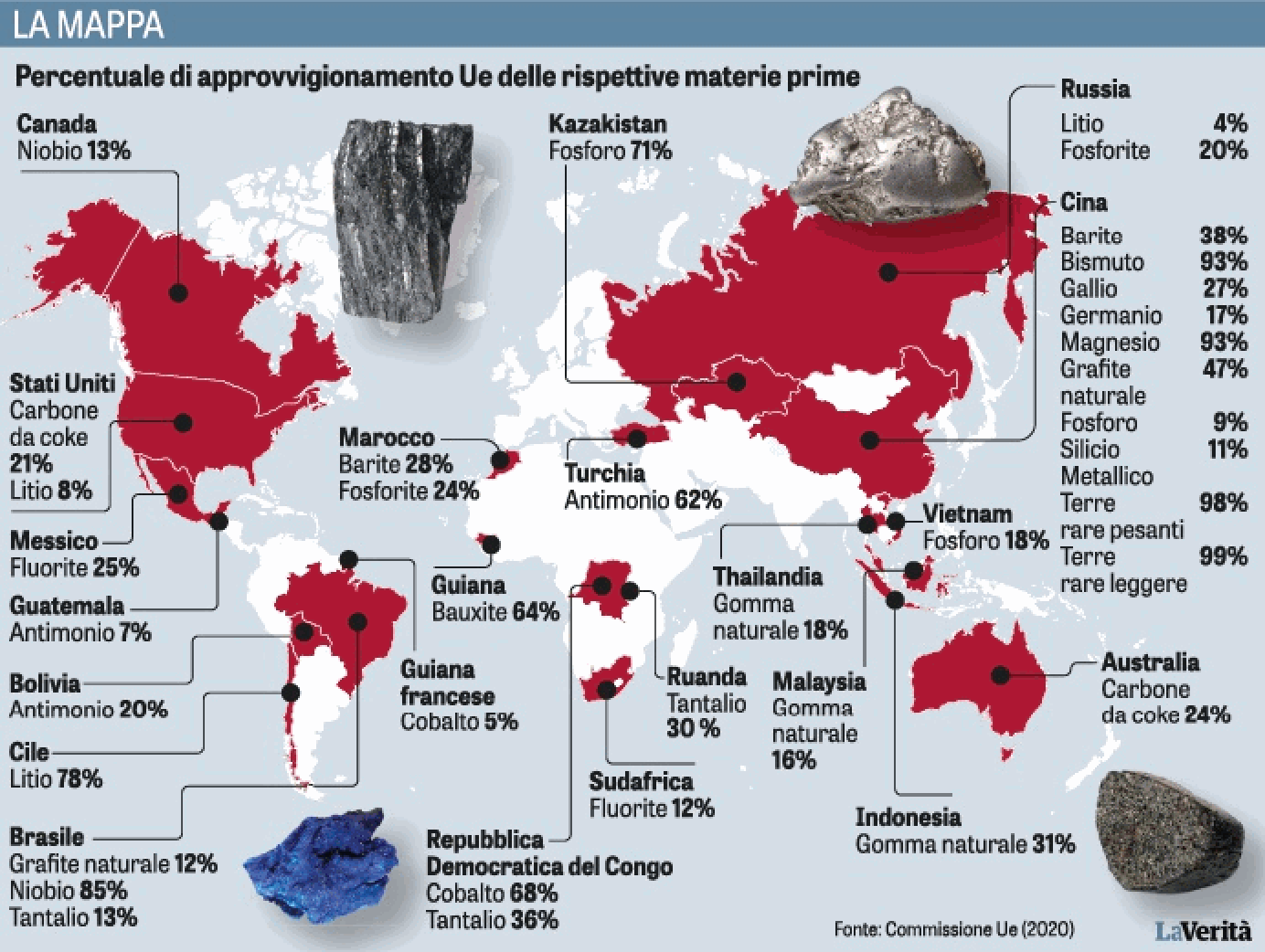
Not to mention that this will replace the dependence on oil with dependence on Chinese-owned minerals. The EU-mandated mass switch to electric requires essential raw materials like lithium, which Europe lacks. Map: the percentage of the said materials imported in the EU from the respective countries.
It was a terrible idea to get born in Europe. This continent is dying, and the future probably belongs to the third world, even if under Chinese ownership, or maybe just to a few Asian countries.
Back to our COVID-dominated lives
🔴 I won’t comment on how every single European country has its own COVID-19 rules for incoming and outgoing people (regarding the tests, the vaccination pass, the quarantine) that change far too often, so that people simply cannot plan a trip or a holiday. I won’t comment much on how their internal policies are utterly inconsistent, but I’ll shortly mention Britain, though.
In the middle of a stupid pingdemic that forced too many people to self-isolate, leading to shortages and to 999 calls being answered after more than 15 minutes, the UK government has decided to let the virus spread among young people. However, it’s not just the number of suspected contacts and the number of positive cases that are increasing: admissions to hospital are up more than 30% and there’s been a 50% increase in deaths over the last week or so. This is going to be funny, but they wanted to ease the restrictions, and so they did.
🔴 Here’s a topic discussed in extenso in the video of July 20, 2021, Les Jeudis de l’IHU – Conflits d’intérêts – Pr. Didier Raoult.
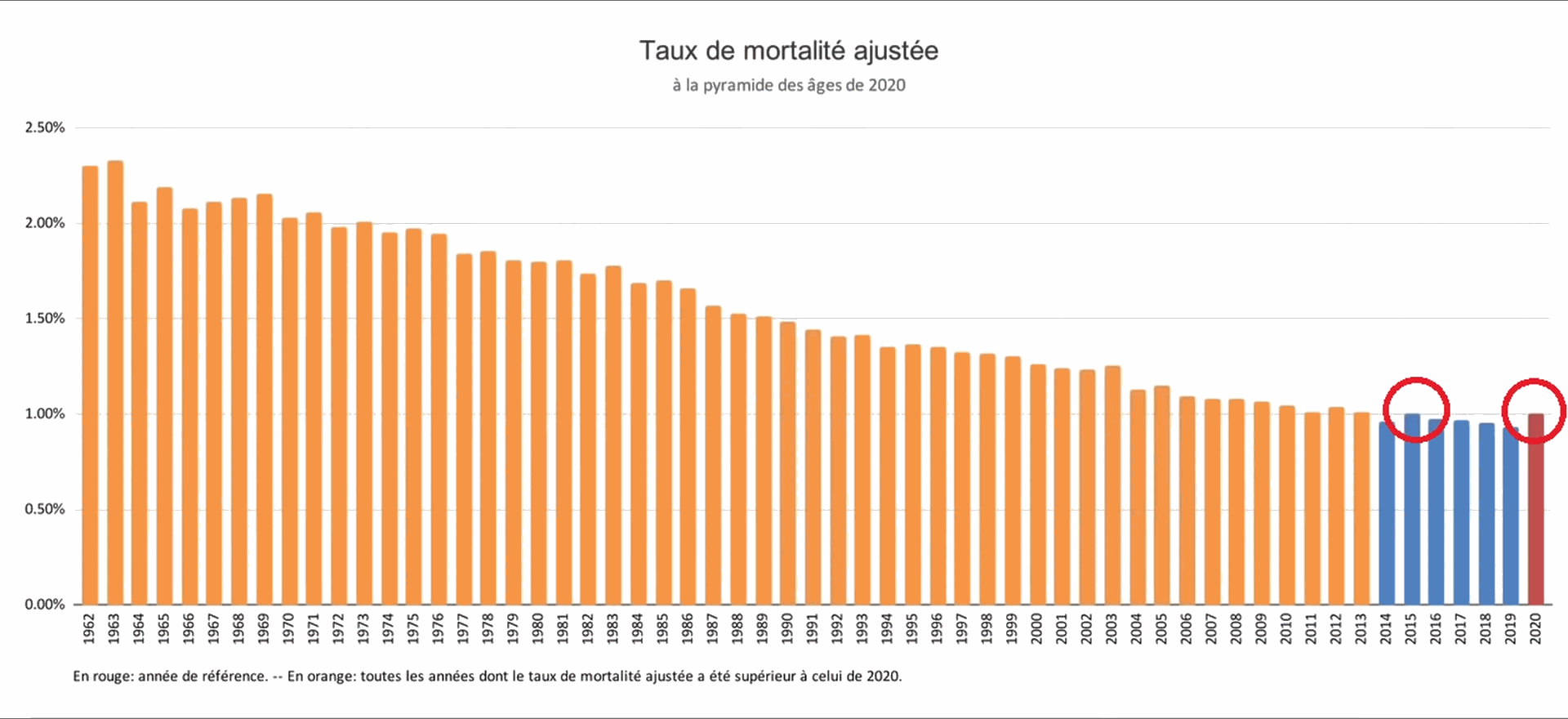
The general mortality has been exaggerated in the official reports, probably to make people more scared of this virus. The French National Institute of Statistics and Economic Studies (INSEE) published back in March the report Avec la pandémie de Covid-19, nette baisse de l’espérance de vie et chute du nombre de mariages. A sharp drop in life expectancy didn’t actually happen, and this official fake news is debunked on AgoraVox in L’arnaque de la chute de l’espérance de vie.
They simply manipulated the data, willfully lying with statistics. First of all, when someone dies at the age of 20, a life expectancy of more than 60 years is lost, but when someone dies at 88, and they already had a life expectancy of less than one year, close to nothing is lost. There are other deliberate miscalculations, but the reality is as follows: even if the mortality for 2020 is slightly higher than the one for 2019, it’s at the same level as in 2015, and the mortality levels for 2014-2020 are all smaller than the mortality in any of the years 1962 to 2013, at least in France!
Sure thing, some people died of COVID-19 complications, some others died for delays in the treatment of severe conditions such as cancer and heart conditions, but on the other hand, the hygiene measures and the partial lockdowns have contributed to a decrease in the deaths from other infectious diseases, and from road accidents. Overall, 2020 wasn’t such a bad year, if we don’t count the diminishing mental health of most people.
🔴 With a certain delay, I then watched Didier Raoult’s video of July 13, 2021, Le variant Delta & le futur des vaccins. This time, Professor Raoult shocked me with a sudden praise for the Chinese vaccine CoronaVac by Sinovac! Funny thing, more recent news claim that Antibodies from Sinovac’s COVID-19 shot fade after about 6 months, so a third booster shot is required, but the thing that charmed Didier Raoult was a study published on July 7, 2021, Effectiveness of an Inactivated SARS-CoV-2 Vaccine in Chile.In this study, the effectiveness of the Chinese CoronaVac/Sinovac has been evaluated on a cohort of 10.2M people (out of a population of about 19M). The results were as follows:
- 65.9% for the prevention of Covid-19
- 87.5% for the prevention of hospitalization
- 90.3% for the prevention of ICU admission
- 86.3% for the prevention of Covid-19–related death
This is great news in itself, but similar results should be obtainable with other vaccines too, especially the mRNA ones (Pfizer’s and Moderna’s), and AstraZeneca’s. What’s the catch?
Professor Raoult doesn’t like how the aforementioned vaccines have severe reactions in some people, and considers that, while the emergency use authorizations made sense for the so-called vulnerable groups, using the same vaccines for mass vaccination is not the right thing to do. What he would prefer is a fully traditional vaccine made of several dead variants, the way they do it with the flu vaccine (despite the flu vaccine being a hit-and-miss, with an efficacy not greater than 50-60%). But I thought the Russian Sputnik-V was also a “fully traditional” vaccine?! Well, maybe it is, but there aren’t many studies about it.
Either way, Professor Raoult didn’t vaccinate himself (he always dodged the question, claiming it’s a private matter, but in fact he didn’t have the couilles to admit he refused to get vaccinated). I suppose he still relies on HCQ.
A more recent study, published on July 22, 2021, Prevention and Attenuation of Covid-19 with the BNT162b2 and mRNA-1273 Vaccines, covers BNT162b2 (Pfizer–BioNTech) and mRNA-1273 (Moderna). Unfortunately, the cohort is tiny: 3975 health care personnel, first responders, and other essential and frontline workers.
- SARS-CoV-2 was detected in 204 participants (5%), of whom 5 were fully vaccinated, 11 partially vaccinated, and 156 unvaccinated (the 32 participants with less than 14 days after the first dose were excluded).
- Adjusted vaccine effectiveness was 91% with full vaccination and 81% with partial vaccination.
- Among participants with SARS-CoV-2 infection, the mean viral RNA load was 40% lower in partially or fully vaccinated participants than in unvaccinated participants.
- Among participants with RT-PCR–confirmed SARS-CoV-2 infection, only 25% of those who were partially or fully vaccinated reported febrile symptoms, as compared with 63% of those who were unvaccinated; the risk of febrile symptoms was 58% lower with at least partial vaccination.
- Vaccinated participants also reported 6.4 fewer total days of symptoms and 2.3 fewer days spent sick in bed with Covid-19 than unvaccinated participants.
I don’t like how this time they don’t give a precise definition of the term effectiveness. It’s about effectiveness in preventing what? Severe symptoms? ICU? Death? To me, the only relevant result is the one put in bold, about the fever, and it’s good, but nothing like the “big numbers” of 91% or 81%.
🔴 A last topic from Didier Raoult’s weekly video, the untrustworthiness of the studies. This is far from being a novel issue (see e.g. §4 here), but this time he specifically mentioned an article from March 8, 2021, Epistemic Corruption, the Pharmaceutical Industry, and the Body of Medical Science. It’s more than just bogus studies: it’s about conflicts of interests and corruption!
I liked a quote from the article:
Each of us is born with a share of purity, predestined to be corrupted by our commerce with mankind, by that sin against solitude. — Cioran 2012* [1949]
*Cioran, E. (2012). [1949] A short history of decay. Editor R. Howard (New York, NY: Arcade Publishing).
🔴 Speaking of conflicts of interests, a video from July 19, Les Jeudis de l’IHU – Conflits d’intérêts – Pr. Matthieu Million, covers … um … the hydroxychloroquine. It’s the point of view of a clinician using HCQ for 10 years. It tells the story of the LancetGate and of 56 studies on the HCQ and 4 studies on remdesivir.
You can find a list of the published studies here, with an extra list of pre-print ones on a separate tab. The study Predictive Factors of Clinical Assays during COVID-19 finds correlations between potential conflicts of interests and the inefficacy of the HCQ:
Among the 6 studies on remdesivir, both positive and negative predictive value of potential conflict of interest with remdesivir were 100%. All 5 studies with a conflict of interest declared or not declared were in favor of remdesivir, the only study without conflict of interest reported no benefit with remdesivir.
Among the 56 studies on HCQ, the following criteria were associated with a predictive value > 50% for HCQ efficacy (Table 2):
– Detailed treatment protocol (84%),
– At least one of the main authors expert in the field (affiliated in infectious diseases, internal medicine or pneumology) (76%),
– Control for severity (at least oxygen) (75%),
– Centers and doctors who take care of patients are identified (73%),
– Diagnosis formally confirmed (PCR or serology-based diagnosis) (69%) and
– Control for health status (at least age) (63%).Conversely, the following criteria were associated with a predictive value significantly > 50% for HCQ inefficacy:
– Private data computing company (100%),
– Toxic treatment (100%),
– Potential conflict of interest with remdesivir (73%) and
– Undeclared funding or conflict of interest (66%).The difference of predictive value according to each criterion was significant for
– potential conflict of interest (p = .001),
– lack of detailed therapeutic protocol (p = 0.011),
– toxic treatment (p = 0.013),
– Unknown centers and doctors not known (p = 0.03), and
– private data computing company (p = 0.041).The 18 observational studies with a detailed therapeutic protocol and without a potential conflict of interest had a 100% predictive value for HCQ efficacy (Table 3).
🔴 People keep misunderstanding how elementary logic and statistics work, and they start from a news report that says Vaccinated people make up 75% of recent COVID-19 cases in Singapore, but few fall ill to construct this anti-vax narrative–the example is taken from the Romanian TV station Antena 3.
First, they simply ignore the “but few fall ill” part.
Then, they interpret it as “see, I told you vaccines are useless!”
I covered the misunderstanding of elementary statistics here, with regards to Israel (just above “What is to be done?”), then here (after the fourth green subtitle bullet). But let’s make it even simpler: should 100% of the people get vaccinated, and a vaccine’s efficacy be less than 100%, then 100% of the COVID-19 cases would be from vaccinated people!
🔴 Another misinterpretation in bad faith, also encountered at the same TV station. Wow, “BREAKING NEWS!, the FDA will stop using the RT-PCR tests, but only since Dec. 31, and oh my, they have terrorized an entire planet with unreliable tests!”
The actual news was 4 days old, and it read like this: 07/21/2021: Lab Alert: Changes to CDC RT-PCR for SARS-CoV-2 Testing:
After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only. CDC is providing this advance notice for clinical laboratories to have adequate time to select and implement one of the many FDA-authorized alternatives. …
In preparation for this change, CDC recommends clinical laboratories and testing sites that have been using the CDC 2019-nCoV RT-PCR assay select and begin their transition to another FDA-authorized COVID-19 test. CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza viruses. Such assays can facilitate continued testing for both influenza and SARS-CoV-2 and can save both time and resources as we head into influenza season.
Simply put, they now want to encourage labs to transition to using a test (Flu SC2 Multiplex Assay) that would reliably detect both the SARS-CoV-2 and the influenza virus, which saves money and time. There’s nothing more to say about that.
Who’s for mandatory vaccination?
I am for it, despite the contradictory measures taken by the various central and local governments in Europe. Alabama’s governor’s “it’s time to start blaming the unvaccinated folks” made my day.
In most civilized countries, there are many mandatory vaccinations, despite the lack of a consensus as for which one should be mandatory and which one should be recommended. Despite Germany opposing forced COVID-19 vaccination, for the other communicable diseases, the German immunization schedule is quite heavy:
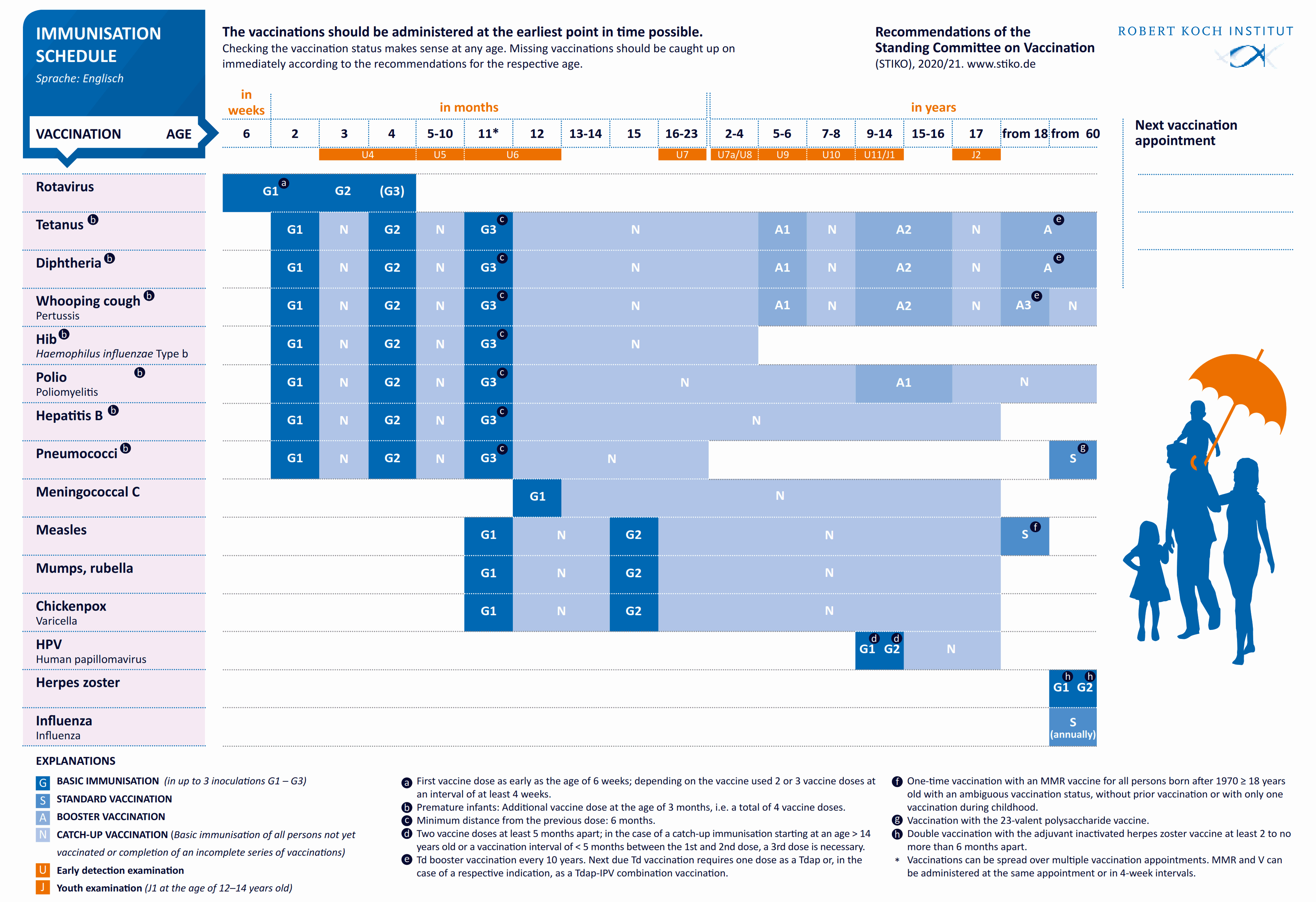
Only the few vaccines marked S (Standard vaccination) are optional.
With COVID-19, it’s a question of public health and even of national security. This is not about people dying, this is about disrupting the functioning of the society, and jamming the health care system.
The real issues are the less-than-perfect vaccine safety, the questionable availability of the vaccine, and the possible discrimination against the unvaccinated. But put it this way: when you travel to some African or Asian countries, you have a list of mandatory vaccines, and a list of recommended ones. You cannot enter some countries without proof of immunization with the mandatory vaccines! Some people have had a hard time for weeks after getting all the required jabs, yet they didn’t complain: they did want to visit that exotic destination, didn’t they?
Now, if every single country would make the COVID-19 vaccination mandatory to all foreign tourists, this would help tremendously. Nobody’s forcing anyone to visit a foreign country, so the “freedom fighters” are free to stay in their fucking country! Most people can live very well without any international travel.
I reiterate my personal belief that this virus, being it Delta or any other Greek letter variant, will gradually become less severe and less lethal, regardless of its contagiousness. But since we’ll all get it at some point, no matter what we do, it’s better to get the jab before we get it for the first time. Currently, the so-called “long COVID” has proven to be able to debilitate even the teenagers, so this is not a joke: our bodies don’t know this Chinese virus, and the reactions can be severe or even lethal.
Would the Chinese or the Russian vaccines be any better than the Western ones? Russia and China being “the Devil,” I didn’t hear many debates on that one.
What I’ve heard were lamentations on why, oh why are they torturing the kids, and why those 12-17, if not those 2-11 in some countries? Simply put, for any drug, 12 is a threshold age between childhood and adolescence; then, no matter what they used to say, and respiratory disease is transmissible via kids and teens, so here you have the explanation. (I wonder how they decide on drugs for ages below majority, or below 14 in certain jurisdictions, as I expect minors to be legally unable to participate in medical experiments.)
The $64,000 Question: are the powers that be preparing a complete relaxation of the measures, being them aware that their subjects wouldn’t stand much more? If that’s the case, and people will be left to their own devices, why are the authorities playing the tough guy right now?
We’re living such unpredictable times…
Update 1: Everyone is stupid these days, especially the British government
‘Infuriating’: British expats in France slam UK’s quarantine decision:
For the 148,000 British expatriates living in France, the UK’s decision to lift its quarantine requirement for fully vaccinated travellers from all EU countries except France was hard to take.
The 10-day mandatory self-isolation makes it almost impossible for them to visit their families in the UK, especially for those who have a job in France and little holiday time.
…
British authorities waived on Wednesday their 10-day self-isolation requirement for travellers from amber countries — which include the US and EU member states — as long as they are fully vaccinated against COVID-19.
But the measure, which comes into force on August 2, does not include France, which the UK has classed as “amber plus”, citing the Beta variant as a concern
The UK is meanwhile on France’s “orange” category, meaning that fully vaccinated people can travel to France without having to quarantine upon arrival.
Update 2: The mystery of the relative immunity of children against COVID-19 has been solved
The mystery of why children become infected with SARS-CoV-2 less often and less severely than the adults seems to have been solved. The answer stays in a molecule of the respiratory tract, neuropilin-1 (NRP1), which is essential for the SARS-CoV-2 virus to spread in the body, and which is much less active in children. The discovery has been made by the researchers of the University of Naples Federico II.
Front. Pediatr., July 28, 2021: Age-Related Differences in the Expression of Most Relevant Mediators of SARS-CoV-2 Infection in Human Respiratory and Gastrointestinal Tract
The lower severity of SARS-CoV-2 infection observed in children may be due to a different expression of nasal NRP1, that promotes the virus interaction with ACE2.
Further reading:
June 29, 2021: Targeting neuropilins as a viable SARS-CoV-2 treatment
We conclude that the central roles of neuropilins in vascular, neural, and other pathways may render it a less suitable target for treating SARS-CoV-2 than agents that target its binding partner, the viral spike protein.
…
In summary, while neuropilins are an exciting potential target for SARS-CoV-2 therapeutics, we should tread carefully interfering with so central and ubiquitous a receptor, with key roles in vascular and neuronal development and dynamics, and in pathologies ranging from cancer to ischemic disease. However, understanding the involvement of NRP1 in viral entry, and how the structure of NRP1 governs this, may help in design and testing of other effective therapeutic antiviral approaches.
April 26, 2021: A bird’s eye view on the role of dendritic cells in SARS-CoV-2 infection: Perspectives for immune-based vaccines
COVID-19 pathogenesis is still not fully elucidated, while increasing evidence suggests that disease phenotypes are strongly related to the virus-induced immune system’s dysregulation. Indeed, when the virus-host cross talk is out of control, the occurrence of an aberrant systemic inflammatory reaction, named “cytokine storm,” leads to a detrimental impairment of the adaptive immune response. Dendritic cells (DCs) are the most potent antigen-presenting cells able to support innate immune and promote adaptive responses. Besides, DCs play a key role in the anti-viral defense. The aim of this review is to focus on DC involvement in SARS-CoV-2 infection to better understand pathogenesis and clinical behavior of COVID-19 and explore potential implications for immune-based therapy strategies.
Update 3: A joke with God
Bigotry kills. July 26, 2021: 34-year-old California man who mocked COVID-19 vaccine on social media dies of virus:
Three days before his death, Harmon tweeted: “If you don’t have faith that God can heal me over your stupid ventilator then keep the Hell out of my ICU room, there’s no room in here for fear or lack of faith!”
Before his hospitalization, Harmon had made fun of vaccination efforts on social media.
“I got 99 problems but a vax ain’t one,” he said in a tweet last month.
On July 8, he posted: “Biden’s door to door vaccine ‘surveyors’ really should be called JaCovid Witnesses. #keepmovingdork.”
One of the comments to the article reads as follows:
Reminds me of the guy on a flooded roof praying to God to save him.
He therefore rejected help from a man in a boat, and later another. He was even offered an airlift.
In his drowning moments, he prayed: “Why did you not save me?” God replied: “I sent two boats and a helicopter.”
For those of a religious bent, the Covid vaccines might well be considered gifts from God, delivered through the incredibly educated and well-executed vaccine development. Since no one has credibly claimed to hear the creator speak to them in a couple of millennia, this could be claimed as the wondrous ways in which they work. Mocking the results would be missing the point, I’d think.
Te vaccinasi? Sau bagi HCQ ca idolul? 🙂
2nd Pfizer on July 15. You missed this part: