We Want COVID! (Re-Updated)
I had to interrupt whatever I was doing studying something else, to express my anger against the stupidity of my fellow Europeans. THEY DO WANT COVID! They really cannot live without it!
§1. “Fighters for freedom”
I didn’t deem it appropriate to comment on the mass stupidity displayed the other day by loads of stupid Europeans who demonstrated on the streets of major cities in France, Italy, Germany, and other countries against the “Green Pass” aka “pass sanitaire” (health pass) aka vaccination pass. Such people reject the conditioning of some activities by the vaccination status, but most of them also refuse to get vaccinated. Furthermore, they believe compulsory vaccination is totalitarian, and vaccination of teenagers and kids even more so. As expected, they clashed with the police and, also as expected, in France and in Germany there were cases when the police used unnecessary violence (there’s also been a death). It has to be noted though that the demonstrations were quite violent, and the police might have been under excessive tension and fearing for their lives.
In such times, I’m sorry I was born in Europe, because what we’re experiencing now is the death of the European civilization, and I’m so unhappy I know what they’re destroying right now. Were I born in Asia, I’d have been impervious to this phenomenon. In Japan and in South Korea, one couldn’t possibly see such immensely stupid proof of mass idiocy. Europe is simply suicidal, and North America isn’t any smarter.
In mid-July, 99.5% (99.2% by other sources) of those dying of COVID-19 and its complications in the US were unvaccinated. To counter those unable to understand basic statistics, I’ll add: should 100% of the people be vaccinated, 100% of the deaths would be from vaccinated people, but right now, with vaccination ratios of 40-50% of the populations of major Western countries, when 99.5% of those who die weren’t vaccinated, that has a stark, visible meaning: you’re stupid to refuse the vaccine!
Let’s compare identical cohorts of vaccinated and unvaccinated, and move to England: the mortality of the Delta variant in people 50+ is:
- 0.26 in 100,000 fully vaccinated people
- 1.14 in 100,000 partially vaccinated people
- 4.89 in 100,000 unvaccinated people
You’re still stupid.
§2. “We want COVID!”
Checking on the website of the Stuttgart Airport, a relatively modest airport (the sixth busiest airport in Germany, and having a single runway 07/25), I noticed a stunning fact. While Spain (and its islands) and Greece are “code red” from a COVID standpoint…
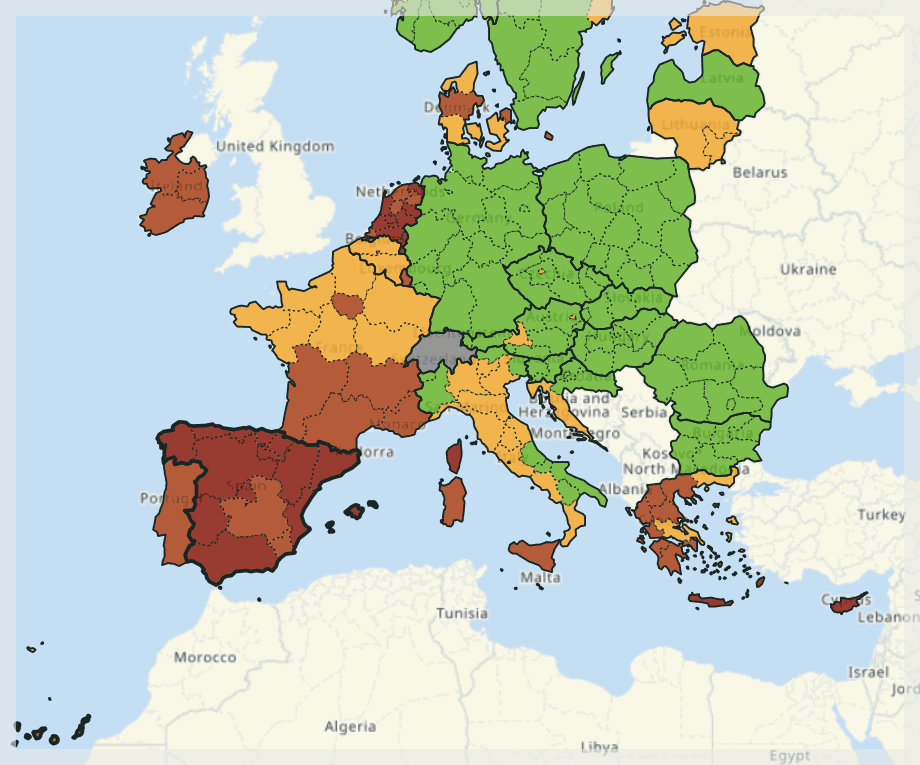
…here are the flights to these destinations scheduled for Thursday, August 5, 2021:
Spain and Spanish Islands:
- PALMA DE MALLORCA 6:00
- PALMA DE MALLORCA 6:05
- PALMA DE MALLORCA 6:50
- MENORCA (MAHON) 7:10
- PALMA DE MALLORCA 9:55
- IBIZA 11:20
- MADRID 11:40
- PALMA DE MALLORCA 11:55
- FUERTEVENTURA 12:45
- TENERIFFA (SUED) 13:25
- BARCELONA 15:10
- PALMA DE MALLORCA 22:10
Greece:
- HERAKLION 6:00
- KAVALA 6:30
- KORFU (KERKYRA) 6:35
- HERAKLION 6:50
- KOS 7:00
- RHODOS 7:15
- THESSALONIKI 9:35
- RHODOS 14:30
- RHODOS 14:55
- ATHEN 15:55
- ATHEN 18:55
- THESSALONIKI 19:25
I must be dreaming! In a single day, 12 flights to Spain (of which 6 to Mallorca!) and 12 flights to Greece! And this is not such a big airport.
What’s worse, I have reliable reports that the Stuttgart Airport doesn’t actually check people’s negative tests or “green pass” (the vaccination status), despite having the CovPassCheck app that’s able to scan papers or the screens of CovPass, Corona-Warn or Luca apps for QR codes! They couldn’t fucking care less, because they could not redesign the passenger flows, so it’s crowded and moving slowly, and slowing it down even further because someone lied about a test or about the vaccination would jam everything unacceptably, right? (Fucktards. Shitheads.) The passengers too are irresponsible: in the terminals or during the flight, they pretend they have a drink so that they don’t wear a mask for long periods of time! Fucking stupid and criminal humankind.
Meanwhile, China suspended flights and trains, canceled professional basketball league games and announced mass coronavirus testing in Wuhan, but Europe is busy with vacationing, no matter what!
We, the European civilization, are totally fucked-up, but we cannot stop going to the beach “on the islands”! Our economy was already destroyed by China and other Asian countries (and it was us who asked them to manufacture everything for us!) even before the pandemic. We continue to deny the reality, being focused on aberrations such as the gender theory (with gender identities that don’t match the biological sex, and with transsexual surgery for children); the banning of combustion engine vehicles by 2035; the introduction of the speed limit of 30 kph in most streets of most French (and not only French) cities; and generally with everything that doesn’t matter. This civilization is going to end while we’re at the beach, on e-scooters! (Scooter as in kick scooter or trottinette, not as in moped aka motor scooter, neither as in mobility scooter.)
Well, not quite. The vacationers have first to return home, bringing more SARS-CoV-2 with them.
§3. Ivermectin³
Why Ivermectin³? Well, possibly because this German keyboard includes symbols for the powers of 2 and 3, so it was easy for me to type it 🙂
For some reason, ivermectin keeps coming back in the news.
There is this preprint study, Favorable outcome on viral load and culture viability using Ivermectin in early treatment of non-hospitalized patients with mild COVID-19 – A double-blind, randomized placebo-controlled trial, posted on May 31, 2021, but only made popular on August 2, by The Jerusalem Post. It’s not a retrospective study, but a double-blind one, but the groups of people who received ivermectin (57) and placebo (59) were ridiculously small!
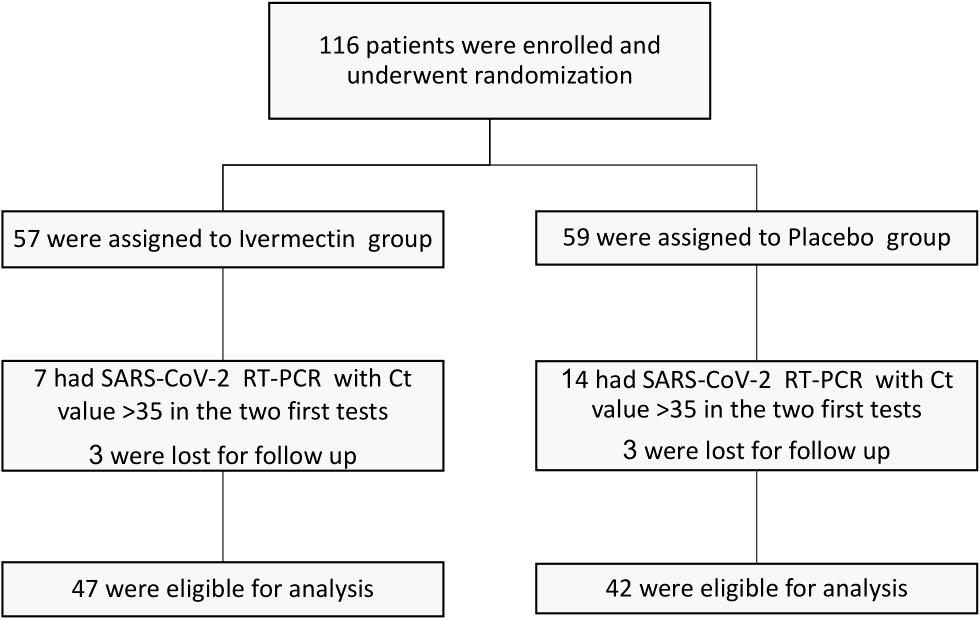
People with Ct>35 are considered negative, and that’s why the final groups were so small.
What this tiny study says? Having the target of measuring the time a patient gets a negative test with Ct>30 (non-infectious level), it compared non-hospitalized COVID-19 patients, asymptomatic at recruitment, receiving ivermectin 0·2 mg/kg for 3 days with patients receiving a placebo.
There were significantly lower viral loads and viable cultures in the ivermectin group; on day 6:
- 72% of the patients in the ivermectin group reached Ct>30
- 50% of the patients in the placebo group reached Ct>30
OK, this is relevant, but what do we do with a single study? Remember how untrustworthy most studies are (see e.g. §4 here, other material here, here, here, and here). And we really lack an intellectually honest debate on most topics, including this one.
Why would ivermectin help, for starters? Compare to this:
- HCQ does modulate the cytokine response, so there goes for an explanation on why it would prevent the destruction of the lungs.
- AZY, despite being an antibiotic, does exhibit some antiviral properties, so there we have a reason too.
But the ivermectin was supposed to kill worms, right? Well, surprise! Regarding this broad spectrum anti-parasitic agent, the aforementioned study starts with these claims:
In the last decade, several in-vitro studies have shown its anti-viral activity against a broad range of viruses, mainly RNA viruses including HIV, influenza and several flaviviruses such as Dengue virus (DENV), Zika, and West Nile Virus.[2-6] Recently ivermectin was tested in vitro against SARS-CoV-2 and showed ~5000-fold reduction (99.8%) in viral RNA after 48 hours.[7] However, it was criticized that the dosing used in the study cannot be achieved with the current approved dose.[8] In addition, ivermectin has anti-inflammatory properties.[9] Since the excessive inflammatory response to SARS-CoV-2 is thought to be a major cause of disease severity and death in patients with COVID-19, [10] ivermectin may have further value in addition to its anti-viral properties.
[1] R. Laing, V. Gillan, E. Devaney, Ivermectin – Old Drug, New Tricks?, Trends Parasitol 33(6) (2017) 463-472.
[2] V. Gotz, L. Magar, D. Dornfeld, S. Giese, A. Pohlmann, D. Hoper, B.W. Kong, D.A. Jans, M. Beer, O. Haller, M. Schwemmle, Influenza A viruses escape from MxA restriction at the expense of efficient nuclear vRNP import, Sci Rep 6 (2016) 23138.
[3] L. Lundberg, C. Pinkham, A. Baer, M. Amaya, A. Narayanan, K.M. Wagstaff, D.A. Jans, K. Kehn-Hall, Nuclear import and export inhibitors alter capsid protein distribution in mammalian cells and reduce Venezuelan Equine Encephalitis Virus replication, Antiviral Res 100(3) (2013) 662-72.
[4] M.Y. Tay, J.E. Fraser, W.K. Chan, N.J. Moreland, A.P. Rathore, C. Wang, S.G. Vasudevan, D.A. Jans, Nuclear localization of dengue virus (DENV) 1-4 non-structural protein 5; protection against all 4 DENV serotypes by the inhibitor Ivermectin, Antiviral Res 99(3) (2013) 301-6.
[5] K.M. Wagstaff, H. Sivakumaran, S.M. Heaton, D. Harrich, D.A. Jans, Ivermectin is a specific inhibitor of importing alpha/beta-mediated nuclear import able to inhibit replication of HIV-1 and dengue virus, Biochem J 443(3) (2012) 851-6.
[6] L. Caly, K.M. Wagstaff, D.A. Jans, Nuclear trafficking of proteins from RNA viruses: potential target for antivirals?, Antiviral Res 95(3) (2012) 202-6.
[7] L. Caly, J.D. Druce, M.G. Catton, D.A. Jans, K.M. Wagstaff, The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro, Antiviral Res 178 (2020) 104787.
[8] M. Bray, C. Rayner, F. Noel, D. Jans, K. Wagstaff, Ivermectin and COVID-19: A report in Antiviral Research, widespread interest, an FDA warning, two letters to the editor and the authors’ responses, Antiviral Res 178 (2020) 104805.
[9] X. Zhang, Y. Song, X. Ci, N. An, Y. Ju, H. Li, X. Wang, C. Han, J. Cui, X. Deng, Ivermectin inhibits LPS-induced production of inflammatory cytokines and improves LPS-induced survival in mice, Inflamm Res 302 57(11) (2008) 524-9.
[10] P. Mehta, D.F. McAuley, M. Brown, E. Sanchez, R.S. Tattersall, J.J. Manson, COVID-19: consider cytokine storm syndromes and immunosuppression, Lancet 395(10229) (2020) 1033-1034.
I did not check any of these studies, but seven of them are from before the pandemic, and a couple of these have extremely relevant titles!
What we’re doing is this:
- Nature, August 2, 2021: Flawed ivermectin preprint highlights challenges of COVID drug studies (no, it’s not “our” study)
- The Scientist, same day: Ivermectin (Still) Lacks Scientific Support as a COVID-19 Drug
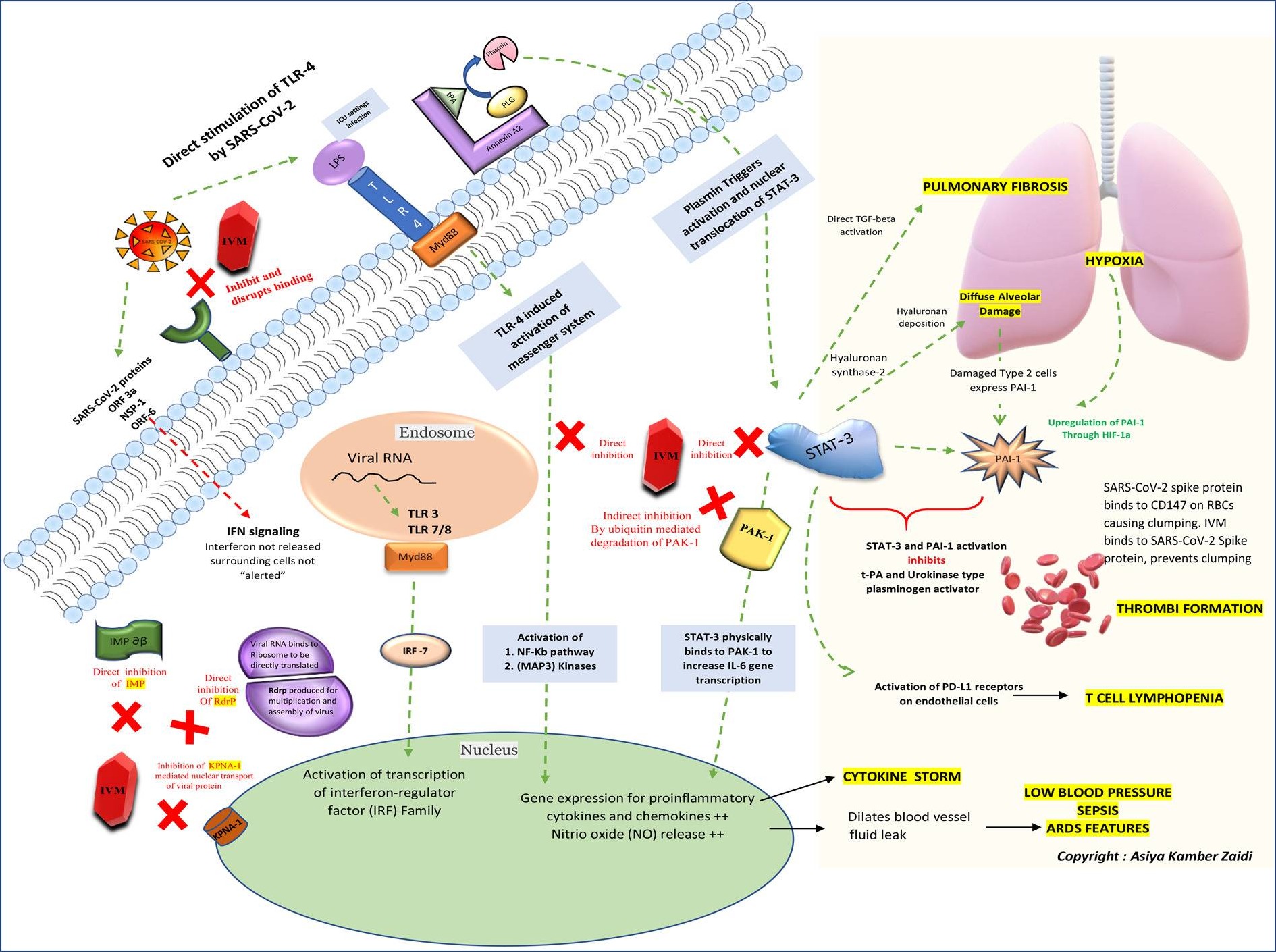
But then, there’s this one: The Journal of Antibiotics (Tokyo), June 15, 2021: The mechanisms of action of Ivermectin against SARS-CoV-2: An evidence-based clinical review article (also on NCBI). And, to no surprise…
22 June 2021 Editor’s Note: Readers are alerted that the conclusions of this paper are subject to criticisms that are being considered by the editors and the publisher. A further editorial response will follow the resolution of these issues.
No kidding. Either way, this meta-study, based on the examination of “the available literature over the years” (67 studies from 1988 onwards!) provides plausible possible explanations of how the ivermectin could work in COVID-19. The explanations are very technical, but I got for you their nice schematic diagram (or whatever it’s called; I suspect schematic diagram only applies to electronics):
I suppose our real problem is that almost nobody is intellectually honest and morally not corrupted, otherwise we’d have had clear, strong, and proven opinions on drugs such as ivermectin, hydroxychloroquine, and others. It might be a romantic idea, or it might be that Didier Raoult (who only loves the hydroxychloroquine and the azithromycin) is right, and the “old (and simple, and cheap) molecules” are more versatile than Big Pharma wants to admit.
Either way, our society is already stuck into a spiral of increasing complexity and increasing costs of everything (legislation and regulation, bureaucracy, electronics and software), probably beyond the point where we’re still able to manage all this crap. I’m terribly pessimistic about the future.
§4. One more paradox, courtesy of Public Health England
As if the conspiracy theories weren’t many enough… I noticed the thing here (as I write this, Twitter didn’t remove it):
😱Delta 🇬🇧 chiffres 💉/non 💉
Le dernier rapport de Public Health England montre que les vaccins Covid-19 AUGMENTENT le risque d’hospitalisation et de décès dus au Covid-19 ‼️Calcul des % à partir des chiffres donnés⏬
1/2 pic.twitter.com/Tmgz0CGpXa— Viv (@CuendetV) August 7, 2021
This kind of people read the rag called The Daily Expose, with articles such as:
- August 3, 2021: Investigation – UK Gov. / SAGE document admits the Covid-19 Vaccines will lead to a variant that kills 35% of people because the jabs do not prevent infection or transmission
- August 6, 2021: NEW – Latest PHE report shows the Covid-19 vaccines are INCREASING the risk of hospitalisation and death due to Covid-19 significantly
The latter is the source for the tweet. This “journal” is abject, and it will continue to be so even when not all the phrases are describing falsehoods. It’s enough to read the comments to their articles, and you’ll notice who their reader base are: people who deny the existence of SARS-CoV-2!
But there is a paradox, though. They base their last shit on this technical briefing:
In this report, the table at page 18 includes such data:
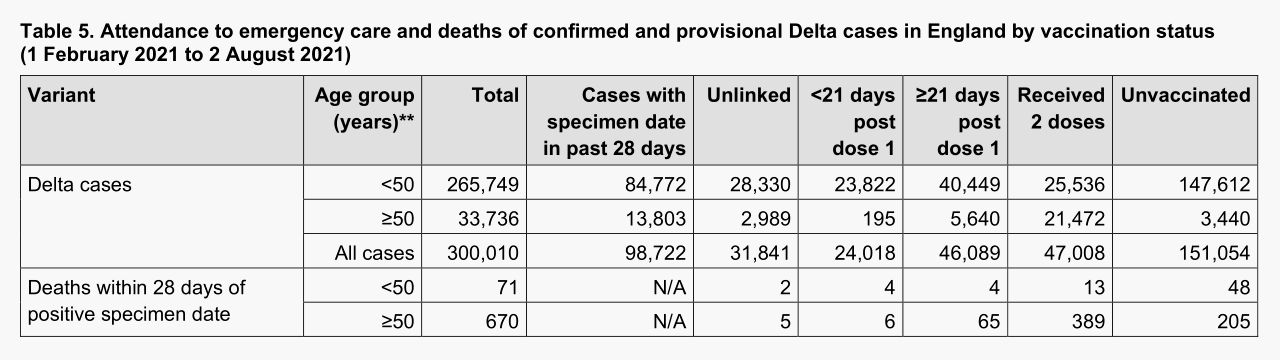
I removed the rows with hospitalizations, because it included several confusing ways of counting them. And here’s the problem:
- Deaths for fully vaccinated vs unvaccinated: 0.855% vs 0.167%
- Even for those younger than 50, fully vaccinated vs unvaccinated: 0.051% vs 0.0325%
It should have been the other way around, right?
Side note: counting what percentage of the hospitalized died (fully vaccinated vs unvaccinated) would be irrelevant even in the best scenario. Why? Because, if the vaccine is highly effective, most people wouldn’t need hospitalization at all. However, those for which the vaccine was useless, say because they didn’t develop antibodies, would definitely develop severe conditions (if they were “defective” relating to the vaccine, then they would certainly be “even more defective” facing the actual virus), so it wouldn’t be surprising for most such people to die. In other words, a highly effective (but not perfect, or not for everyone!) vaccine would decrease the hospitalizations, but would possibly increase the death rate among those who still need to get hospitalized!
First, let’s see what’s stupid in PHE’s approach: they summed all the figures starting from the date when only 0.8% of the population was fully vaccinated, and up to the date when 57.5% of the population was vaccinated! This is so meaningless that I cannot find my words!
- On Feb. 1, when only 0.8% of England’s population was fully vaccinated, almost all the cases would come from unvaccinated people!
- On Aug. 2, when 57.5% of England’s population was fully vaccinated, and many more were partially vaccinated, most cases would come from fully or partially vaccinated people!
One cannot compare bananas and coconuts. They don’t have the same consistency! “Here’s the total number of people who died after having been hit with a fruit, ranging in consistency between a banana and a coconut!”
But there’s a more annoying question. A quick, back-of-a-napkin calculation, showed that even if they separated the cases in time windows of relatively constant vaccination rates (which is practically impossible, but let’s approximate), it’s still difficult to explain the paradox, and to come out with numbers showing a clear advantage of the vaccine. Public Health England have created themselves the basis for a new conspiracy theory without realizing it!
Stupid authorities.
§5. Question for the most adventurous of you: how much should a vaccine “protect against death” to be better than without it?
Let me explain. Previously, I quoted from a study mentioned by Didier Raoult, about the effectiveness of the Chinese CoronaVac/Sinovac in Chile:
- 65.9% for the prevention of Covid-19
- 87.5% for the prevention of hospitalization
- 90.3% for the prevention of ICU admission
- 86.3% for the prevention of Covid-19–related death
Well, the last “protection” is to be defined. What does it mean? Does it mean that 86.3% of the people who get in contact with enough SARS-CoV-2 a load as to become infected, regardless of the presence or absence of the symptoms, at least they don’t die? But… that would mean that 13.7% die, which is much more than the death rate in the unvaccinated people!
There must be some other definition of that effectiveness/protection against, or prevention of death.
What does it mean for a vaccine to have a certain efficacy, after all? The useless WHO only has this stupid article on Vaccine efficacy, effectiveness and protection, in which only the efficacy in preventing the contracting of the disease is vaguely defined:
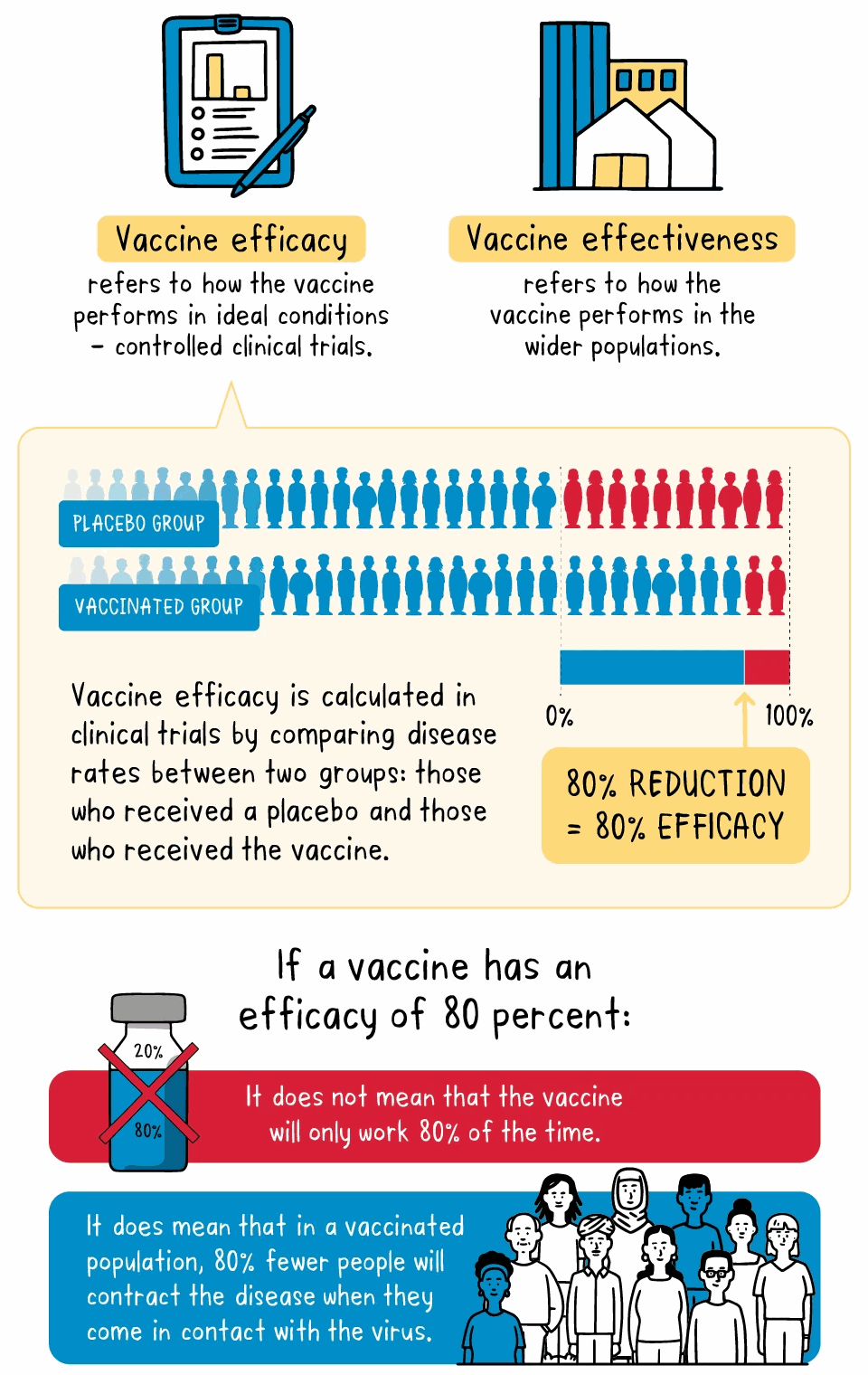
I said vaguely defined, because they don’t say what they mean by “people not contracting the disease”:
- Does it mean “people getting a negative test result while being tested daily”?
- Does it mean “people not having any symptoms or, if they had compatible symptoms, but only then, getting a negative test result”?
- Does it mean that people can really reject a virus the very moment it reaches e.g. the nasal mucosa? I thought that, no matter the vaccine and the targeted virus, it doesn’t work instantaneously, and that someone in contact with a viral load could take at least minutes, if not hours, to defeat the viral load! What if they’re tested right after having being exposed to a viral load? Should positivity being defined as “two successive positive tests”?
Either way, the protection against contracting the disease is probably, in real terms, close to zero as long as the SARS-CoV-2 variants in circulation today are different from the original variant on which the mRNA vaccines have been modelled! Regarding the Delta variant, what everyone expects (or hopes!) from a fully vaccinated status is:
- to prevent, if possible, any significant (medium-severe) symptoms;
- if that’s not possible, to prevent the hospitalization;
- if that’s not possible either, to prevent the admission in the ICU and the invasive ventilation;
- ultimately, to prevent at least the death.
Let’s try to read some more shit on the said efficacy of the COVID-19 vaccines.
BMJ, August 9, 2021: Covid-19: How effective are vaccines against the delta variant?
Data from Public Health England (PHE) reveal that of all the people who died within 28 days of testing positive for the delta variant between 1 February and 19 July, 49% (224) had had two vaccine doses. Almost all of these people, 220, were aged 50 or older.
As the statistician David Spiegelhalter notes, in a population where less-than-perfect vaccines have been distributed widely, one would expect to see deaths occurring among vaccinated people as the virus spreads.
Data up to 4 August from Imperial College London’s React study found that people who said they had received two vaccine doses were half as likely to test positive for covid-19, adjusting for other factors such as age and whether or not they had symptoms. The researchers estimated a 50-60% lower risk of infection from the delta variant if a person was double vaccinated.
“Estimated”… How reassuring!
The picture emerging from various countries does, however, suggest that vaccinated people are more likely to experience symptoms after catching the delta variant compared with earlier forms of the virus.
Data published by the Israeli government suggest that the Pfizer BioNTech jab’s efficacy against symptomatic infection fell from 94% to 64% after the delta variant began spreading in the country.
Ditto. Useful as shit.
Figures from Public Health Scotland published in the Lancet also show a drop in protection against symptomatic illness, from 92% against the alpha variant, which was first detected in the UK, to 79% against delta among people with two doses of the Pfizer BioNTech vaccine. For the Oxford AstraZeneca vaccine, the reduction was from 73% to 60%. Data from Canada, yet to be peer-reviewed, also show a drop in efficacy.
Marvelous.
It’s difficult to compare data from multiple countries because they all have different protocols determining when people become eligible for a covid-19 test, for example. And symptomatic infection can take many forms, from very mild to severe illness.
Toldya! They don’t even know how many people were positive, because in some countries they didn’t test those who didn’t have severe symptoms!
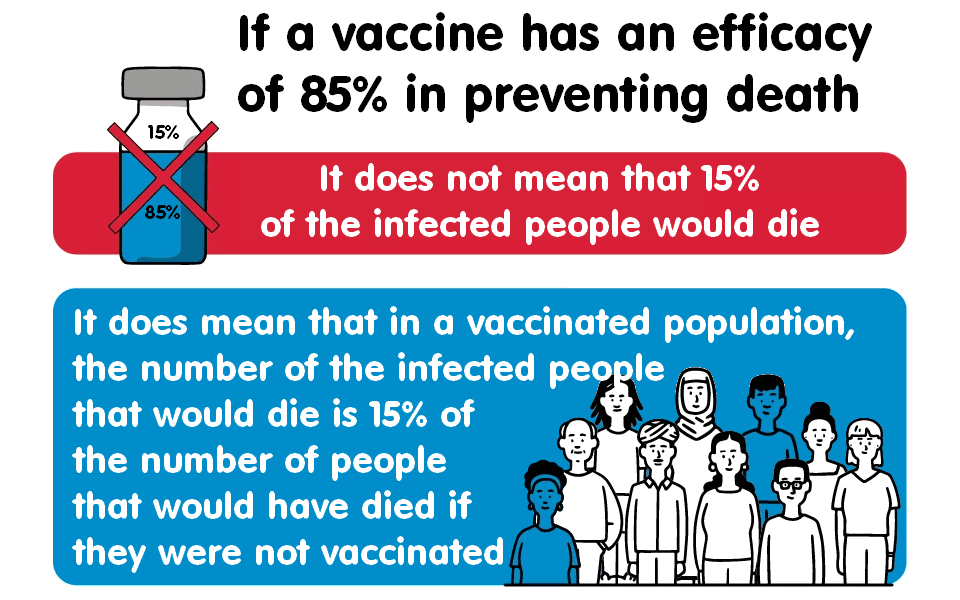
But Riley points out that the PHE data to date are consistent with estimates that suggest—despite these drops in efficacy—vaccines in use in the UK (Pfizer BioNtech, AstraZeneca, and Moderna) all reduce the risk of death by more than 85%, regardless of variant.
Wait, wait! This reduction of the risk of death should mean that if 100 unvaccinated people in a cohort died, only 15 vaccinated people in an equivalent cohort died! That’s what the fucking fucktards should have said in the first place, because this is what people fear the most: death!
Let’s then add a picture that the retards at the WHO failed to consider:
Back to the article:
What about transmission?
…
One yet to be peer reviewed study looked at a single outdoor wedding near Houston, Texas, in April where all 92 guests were required to be fully vaccinated. A couple who had travelled from India later tested positive for delta, with one dying a month later. Of the people they interacted with at the wedding, four became ill with delta. One required monoclonal antibody treatment, but all four survived.A recently released report from the US Centers for Disease Control and Prevention suggests that the viral load of vaccinated people infected with the delta variant is similar to that of unvaccinated people. People remain less likely to become infected in the first place when they have been vaccinated, however.
Lots of “suggestions”: are they established facts, or mere suggestions?!
Neutralising antibodies
It’s not yet clear how the body’s immune system fights SARS-CoV-2. Without knowing for sure what the correlates of protection are, it’s hard to say why a vaccine may be less effective against variants. Evidence is accumulating, however, that the ability of antibodies to neutralise the delta variant is reduced compared with, say, the alpha variant.
It’s not clear how… WHAT?! What are we knowing then?!
A study published in Nature found that antibodies in blood samples (sera) from convalescent patients up to 12 months post-infection were four times less effective at neutralising the delta variant than the alpha variant. Sera from people who had only a single dose of the Pfizer BioNTech or Oxford AstraZeneca vaccines “barely” inhibited delta, wrote the authors.
They did, however, see a neutralising response in sera from almost all people who had received two doses of a vaccine.
Another study on neutralising antibodies, published in the Lancet, found that, following two doses of the Oxford AstraZeneca vaccine, the number of people who had quantifiable antibodies against delta was significantly lower, at 62% (39 of 63), than against the original wild type SARS-CoV-2 (100% of participants).
That may sound worrying, but Akiko Iwasaki, professor of immunobiology and molecular, cellular, and developmental biology at Yale University, says there is reason to be hopeful that people who have had two vaccine doses can still fend off severe disease when infected by delta. This is likely to be in part because of other aspects of the immune system, such as T cells that stimulate B cells to produce antibodies or killer T cells that destroy infected cells in the body.
OK, there is reason to be hopeful. We might not die.
But what kind of efficacy are they measuring in the recent studies? Answer: as many times before, the prevention of (severe) symptoms!
July 22, 2021: Pfizer vaccine 88% effective against delta variant, UK study finds:
Two doses of Pfizer’s COVID-19 vaccine were 88 percent effective against symptomatic disease from the delta variant of the coronavirus, a study published July 21 in The New England Journal of Medicine found.
…
The efficacy against hospitalization and death from the delta variant wasn’t measured in this study.An Israeli study released earlier this month found Pfizer’s shot was just 64 percent effective against the delta variant, but that study’s method has been criticized by some experts, according to The Hill.
August 5th, 2021: Moderna says its COVID-19 vaccine is 93% effective after 6 months, weaker against delta
Being a slide for the investors, which are by definition idiots, they couldn’t be bothered with definitions such as effective against what? “Pipeline momentum” was a much more important newspeak.
§6. The Didier Raoult section
👉 First, an older one I forgot to comment on: Jun 29, 2021: Reprise épidémique chez les personnes vaccinées:
- The biggest blunders that were made during this epidemic were made by the British. As they were a role model for the rest of the world, we have followed them in the error.
- The biggest mortality in the world was in London, which was the beacon of medical research (home of Nature, The Lancet, etc.).
- It was a distortion of the information in the British journals that made them the first victims.
- The place where there were the most of the victims is the place where there are the most of the scientific journals, the most financial resources for health care, more corruption than elsewhere, and more Pharma than everywhere else. It makes it a paradox: it’s inconvenient to be someone considered to be a leader.
- A comparison between the corruption and the mortality in the developed countries reveals a clear correlation: the least corrupt country is Denmark, and it’s one of the countries with the best management of the pandemic. But Denmark doesn’t have any Big Pharma.
- In Marseilles, the mortality in the vaccinated people is comparable to the mortality that the unvaccinated had in the previous waves of COVID-19. But those who die are aged people with preexisting conditions and a low life expectancy. Under the age of 60, the mortality is decreasing. As previously said, the most important is to provide a full treatment to vulnerable people, something they did in Marseilles, but that has not been done in the nursing homes (Ehpad).
👉 Enough blaming the English. Moving forward to Aug 3, 2021: Il n’y a pas de thaumaturge !
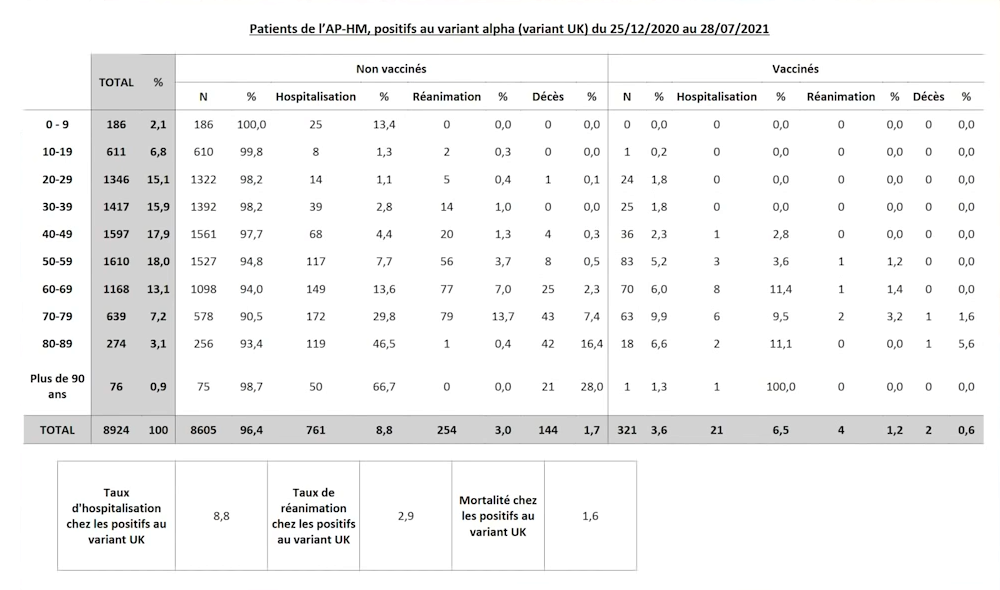
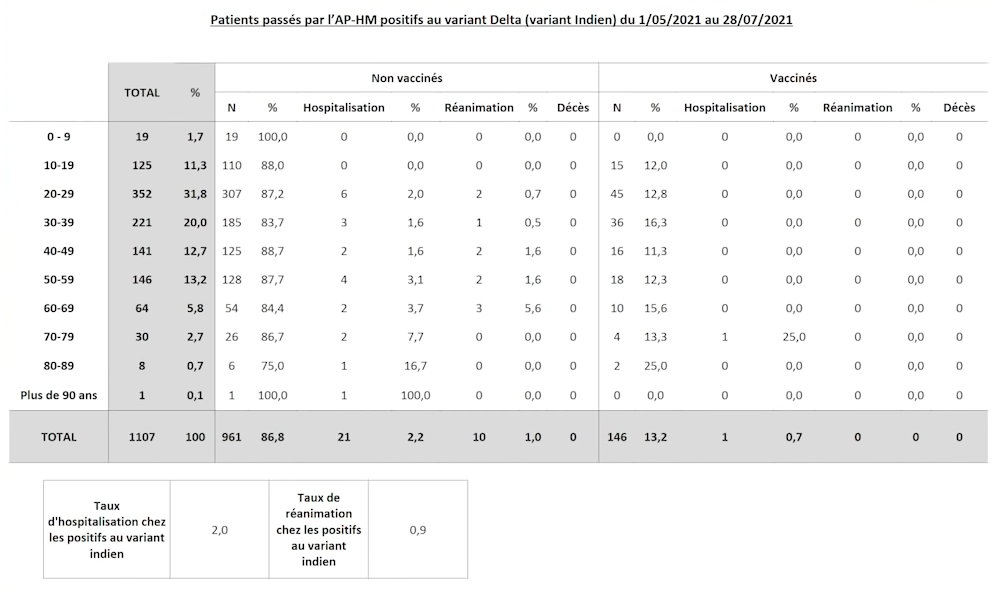
Strictly based on the observations in the AP-HM Hôpitaux Universitaires de Marseille network, where “the positives were real positives and the negatives were real negatives,” what Didier Raoult noticed in the new Delta-prevalent wave of infections is that:
- The proportion of the vaccinated among the infected is higher for Delta than for Alpha: from 8924 infected with Alpha, 3.6% were vaccinated; from 1107 infected with Delta, 13.2% were vaccinated.
- The comparison is however flawed, because the Delta variant is prevalent in young people who got infected in the nightclubs! There are however some older people too.
- This notwithstanding, the Delta variant has led to fewer hospitalizations and fewer admissions to the ICU than the Alpha variant!
- In AP-HM Marseilles, between Christmas 2020 and end-July 2021: Alpha: 8.8% admitted to hospital, 2.9% to the ICU, 1.6% dead. Delta: 2.0% admitted to hospital, 0.9% to the ICU, zero deaths so far.
- Question: If the Delta variant leads to less severe symptoms, is it still necessary to monitor these patients and to give them medical care from the onset?
- Didier Raoult: At the moment, I don’t know.
- The real problem is the aftereffects, or the “long COVID”: there are two complications that happens. The first one is the inflammation of the aorta. The second one is the slowing down of certain brain areas, leading to memory issues and concentration difficulties. The last one affects the youth in great numbers.
- However, a complete medical care (la prise en charge complète), including the hydroxychloroquine where relevant, protects against the “long COVID.”
Some food for thought out there…
§7. The ostrich getaway
Have a video on why the Delta variant is spreading faster:
Giving the prevalence of the “good news”:
- COVID-19 cases in children surge 84 percent in one week
- The Case Against Masks for Children: It’s abusive to force kids who struggle with them to sacrifice for the sake of unvaccinated adults.
- Fit and healthy man, 42, from Southport, who rejected vaccine, dies of Covid
- Israel closes down one more time (green pass, masks for outdoor gatherings, offices at half capacity, quarantine for returning tourists)
- Resist, resign and playing for time: French health workers bid to avoid compulsory COVID vaccination
- Facebook shuts down COVID vaccine disinformation effort that targeted AstraZeneca and Pfizer jabs
- Le gouverneur de Floride poursuit sa bataille contre le masque
- Chinese state media has seized on a Swiss scientist critical of a covid origins probe. The one problem: He might not exist.
…and the fact that, if we’re honest, we don’t know much about COVID,
Could I please go to a planet where such things don’t exist?
I know it’s a myth, but… how could I do this instead, should space travel be impractical?
I’m terribly, terribly tired of all this crap.
P.S.: I already need this posture!



Not a mask in sight. People hugging and kissing. Those who don’t want to, don’t. Which is fine.
It’s like shrugging off a heavy leaden cape and feeling alive again.
It’s the light, whilst Britain looks for ever more control of its own invented darkness.
Resist the regime.❤️
— Laurence Fox ✌🏼🇬🇧✌🏼 (@LozzaFox) August 13, 2021
I’m on a remote island in Greece. No masks anywhere. The bus driver smokes whilst driving, and several young Greeks I have spoken to are not taking the vax. Life is good.
— The Westminster Bubble (@AlexFletcha) August 13, 2021
Several counties across the U.S. have temporarily suspended school because of a surge in coronavirus cases among students and faculty early in the academic year. https://t.co/EOmngyJV7r
— Axios (@axios) August 13, 2021
Re-Update n°1
Sometimes, the governments can really be hugely overreacting:
JUST IN – New Zealand to enter nationwide lockdown after detecting 1st local case for 170 days: “Do not talk to your neighbors.”pic.twitter.com/jCJSU5g0nw
— Disclose.tv 🚨 (@disclosetv) August 17, 2021
Yeah, New Zealand announced it’s locking down the entire country … over one Covid case!
Stay local. Do not congregate. Don’t talk to your neighbors. Please, keep to your bubbles.
Prime Minister Jacinda Ardern said the government had to assume it was the Delta variant, and going for a hard lockdown was better than starting softer and gradually adding restrictions (full video; Axios news report; FEE.org analysis).
The FEE analysis isn’t convincing, because it doesn’t actually explain the madness of the decision:
The Nobel Prize-winning economist James M. Buchanan pointed out that public officials, like everyone else, arrive at decisions based on self-interest and incentives. This idea is known as Public Choice Theory, a field of economics that analyzes political behavior. Though many accept the idea that public servants are motivated to promote “the common good,” Buchanan argued they don’t become altruistic angels upon getting a government job.
OK, so what? They even include a video in which Geoffrey Brennan, Emeritus Professor of Economics at Australian National University, explains the Public Choice Theory, but it still doesn’t ring a bell (at least, not in my case).
Re-Update n°2
Have some fun courtesy of Stephen Colbert, from the show of August 16:
Quick updates.
I’m so pissed off! An update as a comment:
Aug. 31: Judge orders hospital to treat Ohio Covid patient with ivermectin
WTF?! Since when has a judge medical skills? Even if ivermectin might have helped, it’s likely that for a patient “on death’s doorstep” this kind of help would come too late!
Sep. 4: Oklahoma hospitals deluged by ivermectin overdoses, doctor says
No wonder Laurel and Hardy were Americans! Just how stupid can some people be? (It’s depressing.)
OTOH, it’s surreal to say that “gunshot victims were having hard times” [to get to the ER] because of the patients with ivermectin overdoses!
Homo stupidus stupidus is the appropriate name for our species.
IMPORTANT UPDATE! “Oklahoma hospitals overloaded by ivermectin overdoses” is FAKE NEWS! The Guardian lamentably failed for a hoax issued by KFOR, an Oklahoma news channel!
REASON, Sept. 6: The Media Fell for a Viral Hoax About Ivermectin Overdoses Straining Rural Hospitals
Basically, we should stop reading even the most trustworthy mainstream news sources, such as The Guardian. For the UK, they might be credible enough, but for the rest of the world, not so much.
The US is somewhat a special case, with its gazillions of news outlets and a preponderance of fake or semi-fake news, but that’s not a valid excuse for anyone.
Food for thought: Why can’t they just say “Covid is Airborne?” (CDC denies the truth even for mumps.) There is in fact no such thing as miasma, but there is a thing called the airborne transmission of many respiratory viruses! For centuries they believed in the miasma theory and they denied the microbes, but now their conservatism made them deny the fact that beyond the large droplets, SARS-CoV2 (hence COVID-19) is spread through aerosols that can travel far away, beyond the 2 meter “social distancing” norm!
From Why admitting Covid is Airborne is so hard.
Opinion: Guest Essay by Robby Soave, senior editor at Reason: Biden’s Vaccine Mandate Is a Big Mistake (Sept. 10, 2021)
Well, that might be the case, but again, maybe not. I understand that for some people there is such a thing as the primacy of freedom. But consider these facts:
■ For so many infectious/transmissible/communicable diseases, most countries have mandatory vaccination programs for children. Sure thing, there isn’t any consensus on them, so you can have 3, 5, 7, 12 or 17 mandatory vaccines, and there are anti-vaxxers against them too, but still, such mandatory vaccines are a cornerstone of the modern civilization, and a prerequisite to the eradication of certain diseases. If we are to make an exception in the case of COVID-19, it would only be reasonable to base it on the novelty of the vaccines; but again, its social and economic effects are so momentous, that we’d rather not.
■ Not imposing the vaccination nation-wide makes it almost useless. In countries having a federal structure (which I find dumb for US, dumb for Germany, artificial for Belgium, both dumb and artificial for Canada, hypocritical for Spain, acceptable for Switzerland), as long as there aren’t internal borders, the virus is free to roam around. So either you do it, or you don’t do it at all.
■ Governments are limiting the freedoms in many other ways that, in my opinion, are more severe, despite the lack of physically affecting you. You don’t have any real say on the way taxation is made, and some countries enshrined in their Constitutions the legal impossibility of any referendum concerning taxes. You don’t have any real say on what the educational system brainwashes your kids with (here too, the solution is NOT through separate curricula for each US State or each German Land). You don’t have any real say on which drugs or herbs are legal, illegal, or prescription-only. You don’t have any real say on why liquors are so highly taxed or even a State monopoly in some countries. You also have no influence whatsoever on what the secret services in your country are doing. Even with the freedom of speech laws, there is no real freedom of speech, as speech is limited under various pretexts: state secret; trade secret; pornography; privacy of the corrupt individual (to deter whistleblowing); discrimination (the “snowflakes” might get hurt); or pure censorship (including e.g. the N-word and other dash-words). You can’t even change the laws: while means to amend or repeal specific laws exist, the stupidity, slowness, and lack of common sense of most legal systems are immutable. Ultimately, it’s practically impossible to change the political system for the best, it’s impossible to get rid of the traditional, corrupt political parties, and it’s impossible to get rid of the electoral thresholds that discard in some countries any political party that gets less than 7% or 5% of the votes, thus profiting the traditional parties only.
It’s true that for the time being everything seems still questionable about what the various medical and political authorities are undertaking in regard to COVID-19, but I’m afraid that eventually the vaccine will be mandatory in most civilized countries.
In an ideal world, most people would have observed what the authorities RECOMMENDED, so there were no need for compulsion. But with the generalized lack of trust, people disobey even to what’s mandatory, so how would they oblige to mere recommendations?
Well, maybe that’s why we’re fucked up. With no moral authority, things that are forced on people will trigger hostility, resistance, possibly mutiny.
EDIT: Well, maybe this is worth mentioning as an example of observing a RECOMMENDATION: Denmark lifts all Covid restrictions as vaccinations top 80%:
With regard to the vaccine mandate, Louis Rossmann had a video rant: Vaccine mandates coming to employers with 100+ employees.
He’s wrong even when he’s right.
He’s right to consider the possibility of being sued. He’s right to notice that, without a universal vaccine mandate, employees would flee to the employer who doesn’t ask them to be vaccinated.
But, as so many stupid libertarians, he’s wrong to consider it a personal choice. If he’s vaccinated (he is!), but his employees aren’t, any such employee carries a higher risk of infecting another employee or a customer, thus potentially making him liable as an accessory to careless or willful spreading of communicable diseases. This is only a misdemeanor, but still.
He’s however right that modern legislation is absolutely ridiculous and harmful to businesses when he gives the example of the mandate, for businesses with more than 15 employees, to offer training and education on sexual harassment, on what is allowed or what isn’t. Stupid America.
This aside, let’s see what some of his viewers are thinking:
So many reasons to make the vaccination mandatory regardless of the number of employees or contractors, no exceptions! (Indeed, why the USPS is exempted? Why the independent contractors are also having a special epidemiological status? This is preposterous.)
September 15, 2021: Israeli research: 3rd vaccine dose produces 10 times more antibodies than 2nd: Amid talk of 4th dose, serological study at Sheba hospital stokes optimism that booster shot may offer longer-lasting protection than previously thought.
September 18, 2021: National Geographic: Why you may not need a COVID-19 booster yet after all.
Huh?!