COVID-19: Winning the War, but Losing All the Battles
It’s been more than two months since I wanted to write a follow-up to my previous comments on this pandemic, and I never got beyond the title. I finally decided to put a few things there, out of anger.
2020: Next year will be better.
2021: Congratulations, you have completed the tutorial!

This pandemic has so far highlighted the sheer incompetence of the politicians and of the scientists, and the mass idiocy of the Homo sapiens sapiens populace. Now that we have the vaccine (but do we?), things are not going to improve.
Not that soon. Not that fast. Not fast enough.
We will prevail, but how about the costs?
I never thought this will lead to the biggest global crisis since the World War II. Indeed, this pandemic shouldn’t be compared to the 2008-2009 crisis, nor to the Great Depression, but to a world war, due to the extent of the damage created to the economy, to social behavior, to mental health, to everything.
ONE
🟡 There’s no need to tell you: in most countries, this second or third wave is deadlier than the first one. This shouldn’t be unusual, since the Spanish Flu and the Hong Kong Flu also had a second wave more severe than the first one. But with COVID-19, we have tried measures that severely affected entire sectors of the economy, without stopping the pandemic.
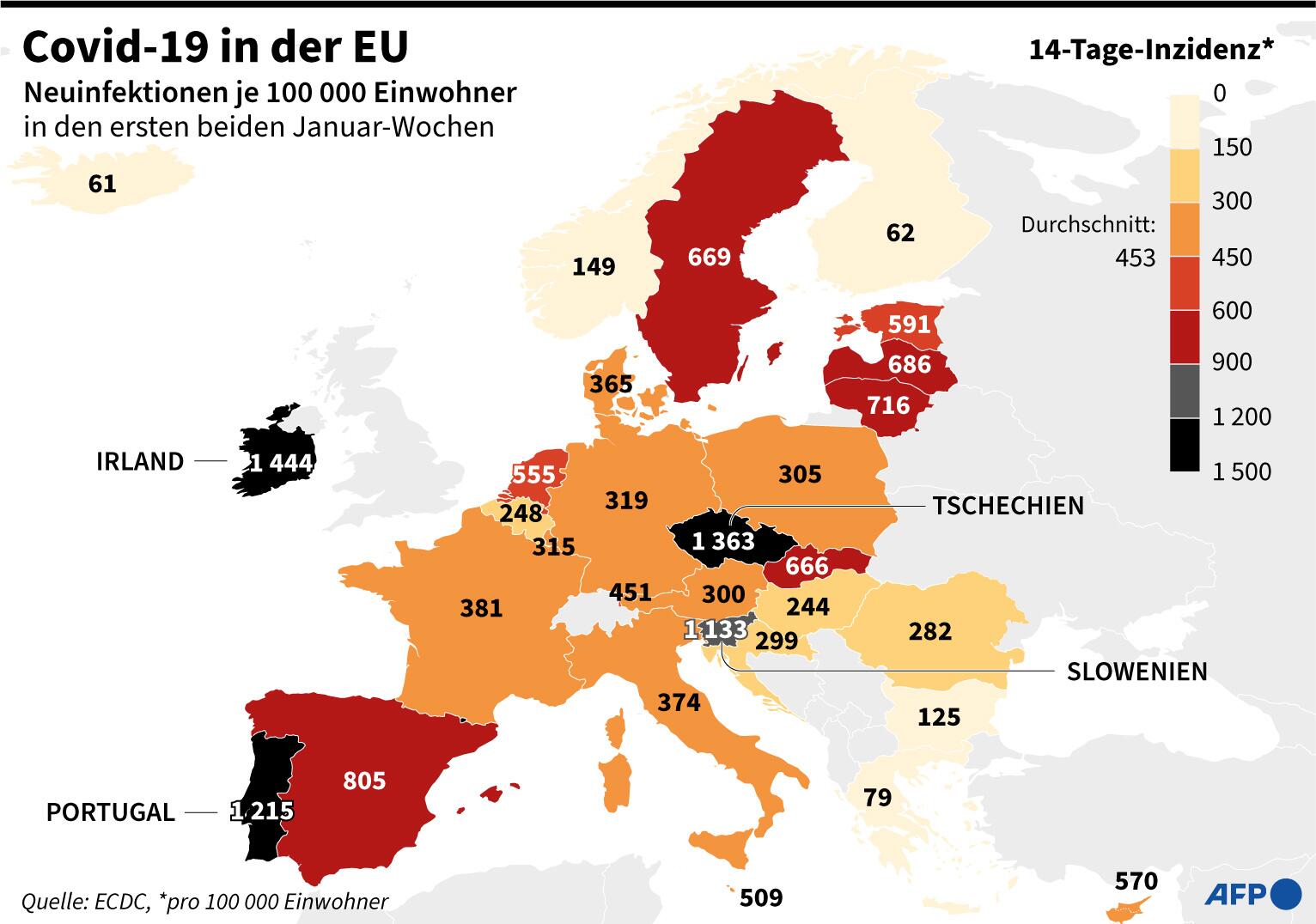
Britain has no data shown in the above graphic, because the European Centre for Disease Prevention and Control decided to ignore them post-Brexit, but we know it’s in a dire state. Even Germany, which is not faring that bad, had January 2021 as the deadliest month of the pandemic so far.
New SARS-CoV-2 variants that seem more contagious, possibly deadlier, and it’s still not known how effective are the current vaccines against them:
- the UK Variant B.1.1.7 (aka 20I/501Y.V1)
- the South African Variant B.1.351 (aka 20H/501Y.V2)
- the Brazilian Variant B.1.1.28 of P.1 lineage (aka 20J/501Y.V3)
TWO
🟡 The “war on vaccines” was an inept “gold fever” to Big Pharma:
- They first secured huge contracts and important development funds from the EU;
- by contract, the vaccine manufacturers were offered civil and criminal immunity in case something wrong happens (I’m flabbergasted that everyone forgot about this clause);
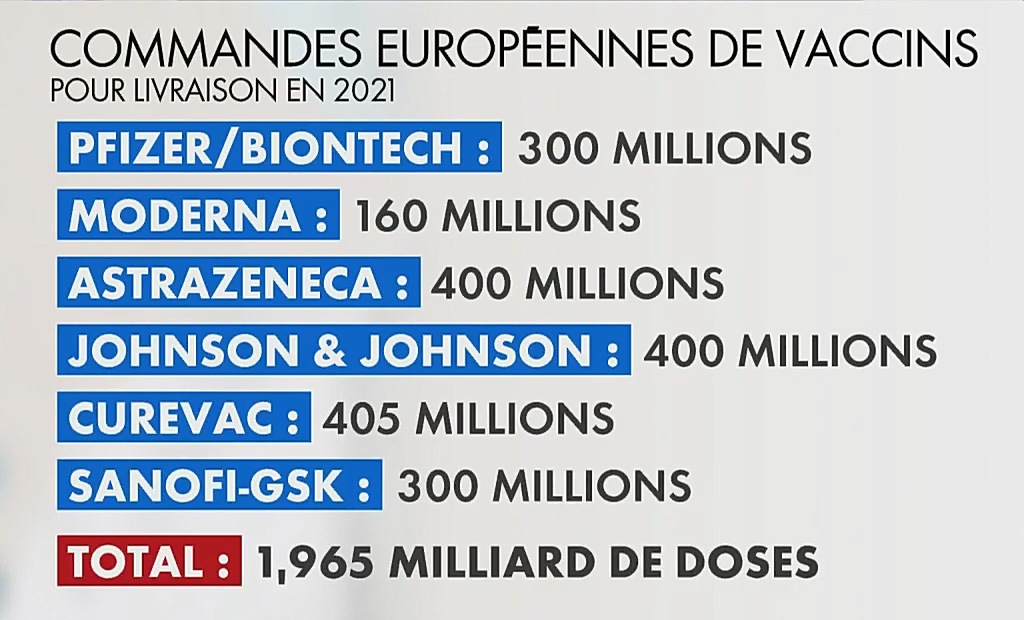
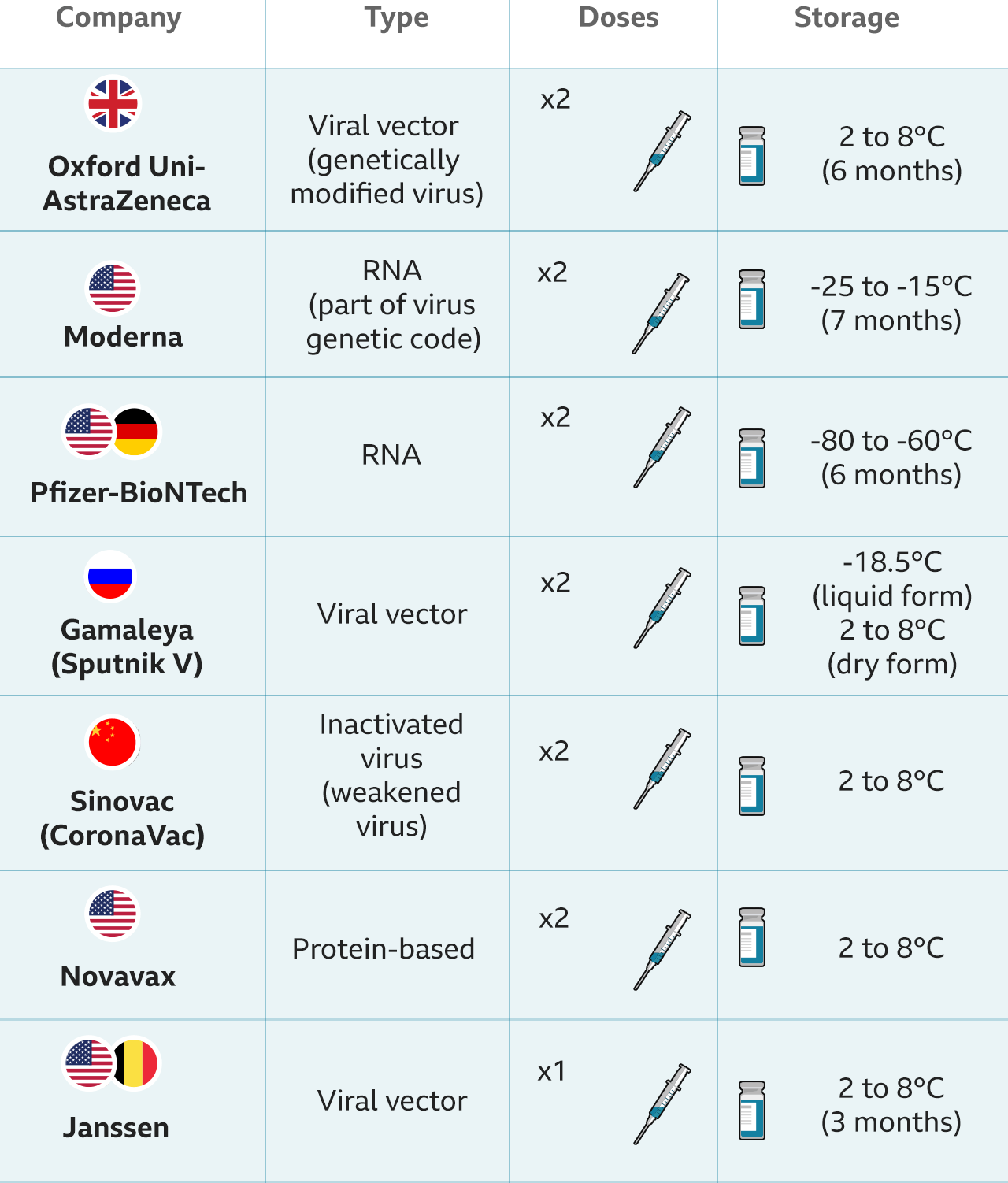
- the contracts were confidential regarding the price to be paid, and only accidentally the prices were revealed (AstraZeneca €1.78, Johnson & Johnson $8.50, Sanofi/GSK €7.56, Curevac €10, Pfizer-BioNTech €12, Moderna $18), which is unacceptable in a matter of public funds and of public health (it’s not just “business as usual”);
- the medicine information leaflets for consumers weren’t available until after the vaccines were approved by the European Medicines Agency (EMA), and with such a lack of transparency, it’s no wonder that hackers unlawfully accessed EMA’s database to read the regulatory documentation submitted by Pfizer/BioNTech (“confidential information about the vaccine and its mechanism of action, its efficiency, its risks & known possible side effects, and any unique aspects such as handling guidelines”–why on Earth are such things confidential?!).
THREE
🟡 It’s no wonder either that some people thought: “They don’t want us to know.” Some other factors contributed to that:
- The first two approved vaccines were of the mRNA (messenger RNA) type, and in the past no such vaccine reached the approval stage. For instance, the original SARS outbreak didn’t attract that much money, and it didn’t evolve into a global pandemic, so any research has been abandoned. Vaccines against rabies, influenza and Zika, all mRNA-based, never made it past Phase 0 clinical trials. It would have helped if the Big Pharma and the powers that be had the honesty to say: “we were cupid and stupid, this is why there weren’t any other mRNA vaccines before.”
- They insisted that these vaccines were possible “because some bureaucratic steps were removed, and some stages were allowed to overlap.” Was that all? Is it just “because of bureaucracy” that sometimes it takes between 12 and 20 years to approve a treatment against cancer? If it’s merely bureaucracy that let millions to die, that such bureaucracy is worse than Hitler, Stalin and Pol Pot! It would have helped to have those bureaucrats say: “From now on, we’ll follow this kind of speedy procedures whenever lives are at stake” (frankly, lives are always at stake).
- It was still a conditional market authorisation, which is not reassuring. Furthermore, the product information leaflet for the Pfizer vaccine has a pathetically succinct chapter “4.8 Undesirable effects”; compare it to the equivalent chapter of any major medicine on any national Medicines Agency of an EU country!
- Not funding the development of a real treatment against SARS-CoV-2 fueled the conspiracy theory that all “they” wanted is to sell billions of vaccines.
FOUR
🟡 Despite the last bullet above, Xenothera’s treatment seems to be effective against the UK, South African, Brazilian, Danish, and Scottish variants of the coronavirus! XAV-19 is more promising than the cocktail of monoclonal antibodies REGN-COV2 by Regeneron that might have saved Trump, and of which Germany has ordered 200,000 doses for a total of €400M (the patients won’t pay a dime of the cost of €2,000 per dose). With the new SARS-CoV-2 variants that will become predominant at least in Europe, effective treatments are a necessity. EMA is now reviewing REGN-COV2, but new treatments are generally facing skepticism from the medical and political authorities; I wonder why.
Cubans also have Itolizumab, an anti-CD6 monoclonal antibody, already in use in May 2020, and it seems to be useful. Nobody cares outside Latin America.
FIVE
🟡 Back to the vaccine. Pfizer/BioNTech can’t produce fast enough. Moderna has to fulfill its obligations towards the US population (should I say US market?). AstraZeneca prefers to supply the UK with jabs, despite the commitments made by the way of an ambiguous contract with the EU. Merck and Pasteur have abandoned their common project of a COVID-19 vaccine for lack of results, with Pasteur following a more traditional approach which may or may not succeed some day. Johnson & Johnson’s single-dose vaccine only has a 66% effectiveness, so I suppose it’s DOA (but the EU has preordered 400M doses, the fools). In the meantime, Russia’s Sputnik V vaccine has an efficacy of 91.6% (“the trial itself was run by a commercial third party based in the Netherlands”), should we trust a study published in The Lancet. I don’t know anything about Sinovac’s CoronaVac, except that Brazil is using it, and Hungary ordered both the Russian and the Chinese vaccines–cold wars are pointless in a matter of life and death, so what matters is to have something that works in most cases.
Also, the “Cold War on vaccines” meant that nobody in the West care to discuss the two Chinese vaccines (even if “they did it,” doesn’t that mean that they know a little more about the virus, and that their vaccine might just work?), and even less of the Cuban one:
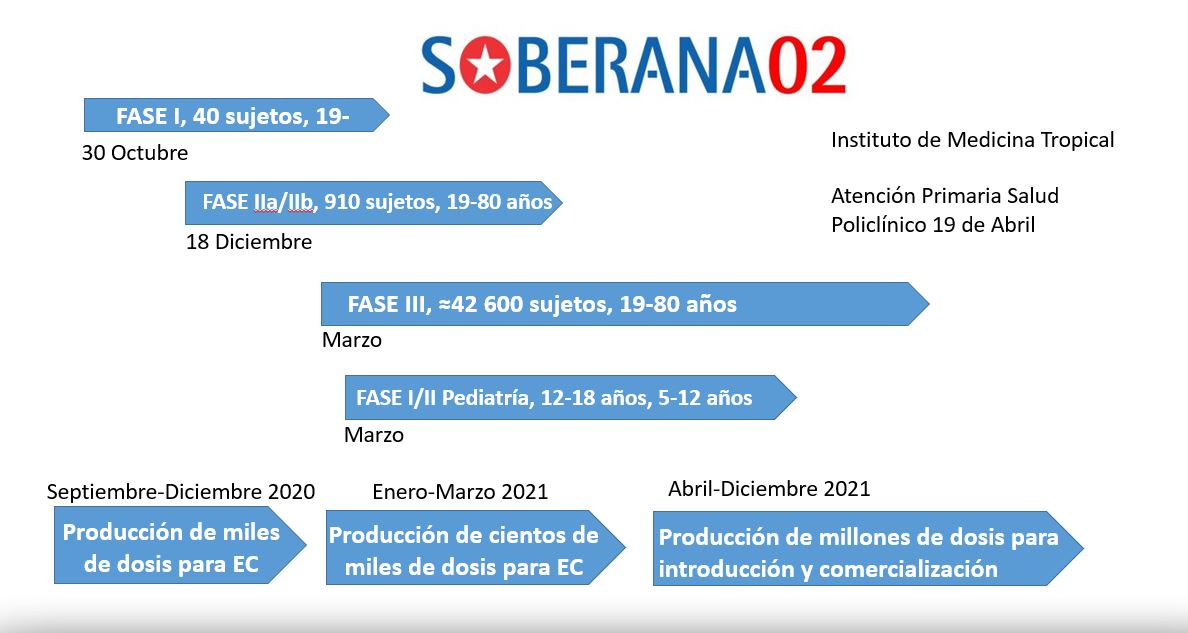
There were two Cuban candidate vaccines, but Soberana 02 entered Phase III clinical trials.
SIX
🟡 The famous “herd immunity” cannot be obtained overnight, and even if 60-70% of the populations gets both shots (most vaccines need a second dose), this won’t magically end the pandemic, except if the rest of 30-40% either die, or they get sick and don’t die. The “herd immunity threshold” only ensures that spreading the virus is very much diminished, so the epidemic fades away. But it’s going to take time. It’s also worth considering that:
- The immunity is not instantaneous not even with single-shot vaccines, and much less with double-shot ones.
- The vaccine might not offer complete immunity to all variants, so flu-like or cold-like symptoms might be experienced by immunized people who encounter a SARS-CoV-2 strain. Death cannot be 100% excluded, as sometimes people die from the regular flu, or rather pulmonary and cardiac complications triggered by a flu.
- No vaccine is 100% effective, not even against the very strain it was conceived against, or made from (when it’s a traditional vaccine).
SEVEN
🟡 Worse yet, while there’s a shortage of vaccines, and so many people who want to get it simply cannot, there are tons of idiots refusing to get vaccinated. Sure thing, vaccination was a hot debate in the latest years already, mostly because the American conspiracy theories have spread throughout Europe via the social networks (including YouTube) and because more and more people become dumbified, which is paradoxical. We’re living in a world where even those with a negative IQ can use smartphones and advanced technologies without believing them magical, and yet there’s an increased distrust in the medical profession.
They say the Czechs are among Europe’s most skeptical when it comes to vaccines as a result of “a mixture of lack of trust in the government, widespread disinformation, propaganda from Russia, and misunderstanding of science.” Only 30% of the Czechs were willing to get vaccinated against COVID-19, a regional study find. But the French didn’t fare much better, with only 31% pro-vaccination by one study, in what’s called “the French paradox: a country with high medicine consumption, but notably low confidence in vaccines.” Well, a French IPSOS survey found 40% of pro-vaccine French in December, and then 54% in January. But is it anything one can trust in France? Both countries are among the least religious EU countries, so at least we know what possible cause to discard. In France, the youth and the women are the most opposed to vaccination, so should we blame the decaying education, and women’s typical lack of logic? (Don’t worry, I’m not just a misogynist, I’m also a misanthrope.) They expect a lot from the state, but at the same time they are very critical of the state, and they don’t want the state to interfere in their private lives. They want socialism without socialism, revolution without revolution, and they would like to punish the guilty politicians, yet they don’t do it: Laurence Fabius, prime minister in the 1980s during the “infected blood scandal,” is unharmed and president of the Conseil constitutionnel, despite having been a murderer. (Thousands of people died of AIDS in France after being given infected blood because the Government delayed the introduction of a US-made blood-screening test in France until a product by Institut Pasteur was ready, and they continued to use the old unheated blood stock while a heated product was available from The Netherlands.)
Of course, it didn’t help that Big Pharma only wants to make money, but being a pharmaceutical company presents a conflict of interests already: if people are healthy, then they wouldn’t buy medicines, so what are Big Pharma supposed to do? Also, it didn’t help that most doctors are known to have prescribed certain drugs for being incentivized to do so by Big Pharma. Finally, nobody trusts the politicians, so when they say something is good for you, the instinct is to assume the contrary.
But it’s ridiculous to come again with the old “vaccines create autism” stupid mantra. Or with new ones, like “mRNA will modify your DNA” and the like. “Thousands of people died from these vaccines”–if so, would Israel commit suicide en masse, knowing that they have vaccinated millions as soon and as fast as they could?
So there was an opposition in the last decade in various countries to the attempts of increasing the number of mandatory vaccines. As a rule, it’s generally accepted that for diseases that are not contagious, a vaccine might be optional, whereas otherwise it should be mandatory to avoid epidemics, and yet…
Again, there are factors to have contributed to the lack of trust in vaccines:
- All they do, the mainstream media, the medical authorities and the politicians, is to repeat ad nauseam: “Vaccines are good, vaccines are good, vaccines are good…”, without trying to debunk in true honesty current and past conspiracy theories. By “true honesty” I mean they should admit that there have been problems in the past with some vaccines or some batches of vaccines. Denying that there have been some problems doesn’t help at all!
- The most pervert anti-vaxxers aren’t only spreading lies, they present half-truths, and they mix true facts with generalizations and lies. Take for one Vaccins, mensonges et propagande, by Sylvie Simon (Thierry Soucar Éditions, 2009), which cites almost 50 anti-vaccination books, but who incidentally mentions a few true facts. There are also a number of “half-honest” anti-vaccination sites, meaning that some of the contents is not “fake news.” But how can the public know what’s true and what’s false if the true incidents can only be found in such places meant to discredit all the vaccines?
- Here’s a true case: when Dr. Salk invented the famous anti-polio vaccines, there were several laboratories producing the vaccine. Cutter Laboratories and Wyeth Laboratories were two such laboratories, and they both produced defective batches. The so-called “Cutter Incident” that in 1955 paralyzed ~200 children for the rest of their lives and killed 10 led to the recall of the Cutter vaccine; that batches included “inactivated” virus strains that weren’t necessarily inactivated. The vaccines by Wyeth were not recalled, and this explains why the cases of polio in the U.S., instead of decreasing, increased by 50% from 1957 to 1958, and by 80% between 1958 and 1959. Since 1963, the Salk IPV vaccine was replaced with Albert Sabin’s OPV (oral) vaccine, using not an inactivated, but an attenuated (weakened) virus… and things improved dramatically! However, the truth has been concealed to the public at the time.
- Another true case, equally troubling: Louis Pasteur lied about a public trial of the anthrax vaccine that helped to make him famous. Details in the Washington Post (1993) and in the NYT (1995).
- Much worse, and quite recently: in Dec. 2017 Sanofi Pasteur was forced to recall its Dengue vaccine, the world’s first vaccine for this disease, for it actually killed about 600 kids! Wikipedia; Scientific American; The Straits Times; from the NPR report:
The French pharmaceutical company Sanofi Pasteur spent 20 years — and about $2 billion — to develop Dengvaxia. The company tested it in several large trials with more than 30,000 kids globally and published the results in the prestigious New England Journal of Medicine.
But halfway around the world from the Philippines, in a Washington, D.C., suburb, one scientist was worried about the new vaccine.
“When I read the New England Journal article, I almost fell out of my chair,” says Dr. Scott Halstead, who has studied dengue for more than 50 years with the U.S. military. When Halstead looked at the vaccine’s safety data in the clinical trial, he knew right away there was a problem.
For some children, the vaccine didn’t seem to work. In fact, Halstead says, it appeared to be harmful. When those kids caught dengue after being vaccinated, the vaccine appeared to worsen the disease in some instances. Specifically, for children who had never been exposed to dengue, the vaccine seemed to increase the risk of a deadly complication called plasma leakage syndrome, in which blood vessels start to leak the yellow fluid of the blood.
“Then everything gets worse, and maybe it’s impossible to save your life,” Halstead says. “A child can go into shock.”
“The trouble is that the disease occurs very rapidly, just in a matter of a few hours,” he adds. “And there’s nothing on the outside of the body to signify the person is leaking fluid on the inside.”
…
Despite these concerns, in July 2016, the World Health Organization went ahead and recommended the vaccine for all children ages 9 to 16.
…
Here’s the problem with Dengvaxia.
Typically, a vaccine works by triggering the immune system to make antibodies against the virus. These antibodies then fight off the virus during an infection.
But dengue is a tricky virus. Dengue antibodies don’t always protect a person. In fact, these antibodies can make an infection worse. The dengue virus actually uses the antibodies to help it spread through the body. So a second infection with dengue — when your blood already has antibodies in it — can actually be worse than the first; a person is at a higher risk of severe complications like plasma leakage syndrome.
In its follow-up study, Sanofi found evidence that Dengvaxia acts like the first infection for a person who has not been previously infected. The body produces antibodies against the vaccine, which have a similar potential for harm.
…
WHO eventually changed its recommendation. The agency now says the vaccine is safe only for children who have had a prior dengue infection.
Instead of admitting that there have been errors and lies in the past, and that sometimes, as with no matter what other medicine, there can be manufacturing errors, the official story says: “vaccines are and have always been harmless, so shut up and obey!“
With such a message, can one wonder that random decisions are taken, such as declaring mandatory vaccination as unconstitutional in Columbia (2017, regarding the HPV), or forcing a mandatory anti-tetanus vaccination in Italy (a 2017 law), when tetanus is not contagious? The public hating of the vaccines is a product of such idiocies!
It would have helped to insist that almost no vaccine today is using live or attenuated viruses or bacteria, but dead ones; unless they’re mRNA-based, in which case they’re totally different, obviously.
If only with the COVID-19 vaccines the full truth were told…
EIGHT
🟡 When the full truth is not told, half-truth and exaggerations are considered “an ideological offensive” against vaccines, in the words of the East StratCom Task Force (ESCTF), the anti-Russia propaganda office of the European Union. Read: Big Lies, Little Lies and Vaccine Vilifications; then Telling Half-Truths is Also Lying; finally, The Battle For Shoulders – Which Vaccine Should Be Injected?.
The problem is that half-truth from interested parties are met with half-truth on the other side.
- “23 Dead in Norway”–that’s a truth, and it was a huge error to give a jab to terminally ill, very fragile people, but it happened! Actually, the final death toll for that bloody incident raised to 29!
- “Ten Dead in Germany after Pfizer Shot”–it happened during the trials, and it wasn’t because of the vaccine (as a matter of fact, 4 of the 6 who died were given a placebo, meaning salted water).
- “One Dead in Belgium after a Pfizer Shot”–correlation is not causation.
The only way to crush such targeted attacks were to have precise reports from the medical authorities, such as: “today 80,450 people received the X vaccine; of them, 893 developed a local irritation, 1230 had a slight temperature increase of no more than 3 hours, etc. etc., and 2 persons had severe allergic reactions bordering an anaphylactic shock, but were given the proper medical attention and face no health risk anymore.”
This is exactly what they do not do. What they did was to tell Twitter, Facebook, and YouTube to remove all the contents that criticized the vaccines or questioned the official policies, abusively labeling such contents as “fake news” without any analysis and no right to contest the decision!
Censorship, the cure-all. The cure that’s worse than the disease.
But remember this: Israel would not commit mass-suicide. And they’re mass-vaccinating!
NINE
🟡 The lack of professionalism and the prevalence of idiocy in this COVID-19 crisis can be suggested by various other facts:
- For a certain vaccine (AstraZeneca, I believe), they* say “we don’t know if it’s effective for people over 65,” simply because the clinical trials only included people 18 to 65. Well, why wouldn’t the vaccine be effective? If anything, it could be unsafe or risky, not ineffective! (By they*, I mean Germany, Italy, France, Poland, Sweden… strange consensus.)
- More generally, if Modena was only tested for 18+, and Pfizer only for 16+, does it mean that there is a magic biological phenomenon to hurt you if you’re 16-17 for Modena or 14-15 for Pfizer, and get vaccinated? Obviously not, but those stupid bureaucrats are too dumb to say “for ages 12+ but below the age we’ve tested for, use extra precautions, and monitor the patient”; similarly, for vaccines not tested for 65+, “patients of 65+ in reasonably good health can be vaccinated if closely monitored afterwards.” Nay, that would mean common sense, and that’s too much.
- Vaccinating those most at risk means e.g. that in Germany, if a couple are aged 79 and 80, respectively, only the one aged 80 was vaccinated in the first wave, and the spouse aged 79 didn’t receive the jab! (Stupid bureaucrats.)
- While the second shot is meant to be given 3-4 weeks after the first one, some governments were trying to push it to 6-12 weeks, which is preposterous! So they don’t know whether a vaccine works at the age 65 as opposed to age 64, but they’re confident that waiting 3 months instead of 1 month would somehow work?! Note that the vaccines that come in multi-pack doses of 5 are already diluted to make 6 doses.
- The countries who refused to impose restrictions or who relaxed the lockdowns prematurely are now among the most affected (UK, Sweden, Switzerland, etc.)
- Some restrictions were imposed without any logic, e.g. “Maskenpflicht” in Germany meant that while on the street, in the cities with an obligation to wear masks in a given time frame, the respective time frame seemed randomly chosen from one of the following ones: 06-24 h, 08-18 h, 08-20 h, 08-22 h, 09-23 h, 10-19 h, 12-20 h. WTF, can’t they have any consistency?
- In countries like Germany, when theaters and cinemas and non-essential stores were closed, churches were open, albeit with limited service. God couldn’t stand to see a closed church!
- As Britain was opening the bookshops at the beginning of December, Germany was closing them. Yeah, so many people were flocking to buy books, more than those watching the Bundesliga. (This government really is stupid.)
- For similar degrees of contamination, you won’t find two countries with an identical policy regarding the way schools should be open or closed, or how should the activity be organized. There’s no consensus on how to balance the importance of education and the importance of public health. If I’m not misinformed, schools in Canada (at least ON and AB) took smart and reasonable measures, including selective testing, smart scheduling, etc.
- The last time when Germany closed the non-essential stores (which are still closed as I’m writing this), they allowed the takeaway eateries to operate. Then they closed them, only allowing deliveries. Later they strengthened some measures, but relaxed those regarding the retailers: whoever was able to offer Abholung-Service aka Click-and-Collect was allowed to be open. Why couldn’t this be allowed all the time?!
- While the real problem was the economy, the German Federal Government issued on Nov. 14 a stupid video targeting the idiotic youth who just cannot stay home without getting bored to death and suffering like heroes: Germany hails couch potatoes as heroes of coronavirus pandemic.
- Many governments didn’t or still don’t have the right to impose lockdowns or further restrictions unless it’s a war! Trump was accused of leaving lockdowns and masks on Governors, but he just couldn’t impose such things! Angela Merkel can’t impose, and she didn’t impose anything either! All the restrictions, even those that seemed uniform nation-wide, were taken by each of the 16 Ministerpräsidents of the respective Länder, after having consulted the Chancellor! Angela simply can’t force anything on the states of the Federal Republic. Even worse, before the new law that has been voted this January, the Swedish government couldn’t impose any lockdown even if they wanted to! This is not democracy, this is idiocy, and suicidal at that.
- There was no “Swedish model” (nor “The Swedish Exception”), and their chief epidemiologist Anders Tegnell is a mass-murderer; a study published on Dec. 22, 2020, revealed that “On Dec 20, 2020, COVID-19 deaths in Sweden had reached more than 8000 or 787 deaths per 1 million population, which is 4.5 to ten times higher than its neighbours. This difference between Nordic countries cannot be explained merely by variations in national cultures, histories, population sizes and densities, immigration patterns, the routes by which the virus was first introduced, or how cases and deaths are reported. Instead, the answers to this enigma are to be found in the Swedish national COVID-19 strategy,” meaning that they did almost nothing, no restrictions at all, but merely some timid suggestions. The death rate per capita because of COVID-19 is higher in Sweden than in France (as of Feb. 7, 2021), and the government still doesn’t impose the wearing of masks! Morons be morons. (Of course, freedom & stuff.)
- The Danish were indeed stupid to kill 10M minks (out of the 17M initially set to be killed), but there is a thing nobody paid attention to: a team from IHU Méditerranée Infection (not Didier Raoult personally) explored “La piste du vison (the mink track)” and that many areas that had huge COVID-19 outbreaks, including Lombardy, host an important number of mink farms! Nobody cared about this study! (Read also this report.) We’re far from understanding how the pandemic has spread so fast, and yet nobody seems to want to know!
TEN
🟡 Mask-gate, although there isn’t any. But after so much quarreling regarding the usefulness of face masks, the authorities decided in some countries that FFP2 masks are recommended or even mandatory.
This should have happened long ago. The idiots were always questioning the usefulness of the surgical masks (OP-Masken in German), which indeed are more effective of protecting the others against the droplets coming from the bearer than the bearer himself, meaning that everyone should wear such masks (and correctly!) to offer protection, while all the time the only solution were to mandate FFP2 or KN95 masks! Instead of that, in most countries even home-made cloth masks were accepted. Morons. (Also, FFP2 masks with valve should have been forbidden from day one, as they offer zero protection to the others, and only protect the wearer.)
The funny thing is this: one year later, the FFP2 masks are still Made in China! Yup. Fucking stupid Western countries, that is.
When Austria mandated FFP2 masks in public transport and shops, guess what? Several supermarket chains made them available for €0.59 since January 21, most likely with subsidies from the government. You know, the famous “right-wing” Chancellor who doesn’t like Islamists; he seems to be quite effective. Also, those masks were Made in Austria! (Normally, FFP2 masks made in Austria were listed at €4.99, or €2.90 at the very least.) In Germany, when Bavaria announced a similar obligation, the price of FFP2 masks jumped to €5.99, with cheaper masks only available online, for about €1 apiece.
Most German Länder only recommend, not mandate, FFP2 masks, but I was able to find at a local online pharmacy FFP2 masks (Made in China this January!) in 20-pc boxes for €20. One week later, FFP2 masks showed up again in physical stores, e.g. DM had 5 masks for €4.95 (also Made in China), but at the tobacconists they’re €2.99 (one week later, €0.99 at REWE, then at EDEKA). Either way, surgical masks at €0.50 suddenly seem too expensive! As for the cloth ones… they just went to the dumpster.
It took a new virus strain (the British B.1.1.7) to persuade the authorities that FFP2 masks should be used. Why, oh why?
Also, they needed the same British strain to conclude that “err… umm… after all, children too can get sick or they can spread the disease, but… err… only with this news strain, otherwise no, they don’t, no matter they do with the regular cold, the flu, and other respiratory diseases!” Idiots. Virologists such as Christian Drosten, who initially opposed everything (masks, lockdown, closing of schools) but now he says, “listen to the experts,” should have their medical diploma revoked!
One more stupidity: in Germany, people from the categories at risk are supposed to receive by mail a voucher enabling them to get 6 FFP2 masks from any pharmacy for only €2. But the pharmacies are reimbursed €6 per FFP2 mask, because the Federal Government has used the market price of October 2020, plus VAT, even though today, certified FFP2 masks can be purchased in bulk for 60-70 cents apiece! So yes, this is a scandal. Besides, why not sending directly the 6 masks to such people instead of sending those vouchers? A legitimate question…

One more question not answered by anyone: despite such masks having been tested and found conforming to the specifications, how can this really be so when such masks (FFP2 or KN95, it doesn’t really matter) have two dashed stripes one can see through?! How can those areas still retain 94-95% of the droplets, despite being much thinner and very different to the rest of the mask? (Nobody seems to care.)

ELEVEN
🟡 This pandemic taught me that even the smartest guys can be terribly stupid sometimes and that even famous doctors can say dumb things. It also made me reconsider the high esteem I had for a number of public personalities, not all of them very famous outside their countries. All in all, I’ve got sated with all the idiotic news from everywhere, so I severely cut the intake of news, but news are like leeches: you chase them out the door, and they come back through the window (this is how a saying runs in French and Romanian, but it’s actually a Turkish proverb). I cannot but learning every single day how stupid are the humans of the 21st century.
Take Prof. Christian Perronne, former President of the Communicable Diseases Commission of the Haut Conseil de la Santé Publique until 2016, Head of the Infectious and Tropical Diseases Department at the Raymond Poincaré Hospital in Garches until December 17, 2020 (when he was forcefully discharged), author of the book Y a-t-il une erreur qu’ils n’ont pas commise ? (Albin Michel, 2020). He’s right in the book when he condemns the actions taken by France’s governments since 2011, when 1 billion face masks were simply destroyed, and during the COVID-19 crisis, but he’s also “chief conspiracy theorist” (and I’m not talking of the hydroxychloroquine). Here’s this guy claiming (in 2021!) that face masks are totally useless, after having repeatedly insisted that mRNA vaccines are gene therapy —something that is entirely false and an aberration (not even Éric Zemmour would have said that; actually, he said exactly the contrary in one of “Face à l’info” shows, while Marc Menant was more skeptical, being a sort of Monsieur Anti-tout)–not to mention that since September he claims there’s never going to be a second COVID-19 wave, unless the Government makes it up! The video about vaccines being gene therapy has been removed by YouTube (here’s a Facebook reference to it), and an article with the same topic has been deleted by Facebook (here’s a reference to it). Christian Perronne might be a competent profesional, despite his war with Big Pharma concerning the Lyme disease (or maybe because of it!), and the persecutions against him for a “crime of opinion” are abject; but when it comes to this pandemic, he’s simply an idiot.
Take Prof. Didier Raoult, which I generally admire, a competent doctor, microbiologist and infectiologist, with great results in various tropical diseases, and who is still right:
- concerning the fact that the combination hydroxychloroquine + azithromycin works great in the initial phase of the disease and also preventively, as it modulates the cytokine response of the immune system;
- concerning the fact that the hydroxychloroquine is generally very safe, having been known for about 80 years (via the chloroquine, a derivative of the quinine) and having been taken by 2 billion people to prevent or treat malaria and, more recently, in the treatment of autoimmune diseases, including lupus (did I mentioned the cytokines, which are responsible for both lupus and severe complications of SARS-CoV-2?);
- concerning the fact that most of the deaths in France (and not only there) happened because the stupid medical and political system told people to stay home and take paracetamol if needed, instead of taking care of them (“la prise en charge”), not only with hydroxychloroquine and whatnot, but also with blood thinners or anticoagulants, antivirals (remdesivir), monoclonal antibodies (rituximab, REGN-COV2), corticosteroids (Dexamethasone), whatever else is required (either protocol-based or adapting to the patient), while monitoring the pulmonary function (at the very least with an oximeter), so that complications be detected at the earliest. We’re now aware of the many complications that arise in most COVID-19 patients; we’re also aware that to have a high survival rate, adequate treatments should be provided as early as possible, otherwise intubated patients only have a limited chance of survival (as low as 25-50% initially, when the protocol they used was for the regular pneumonia); furthermore, because of the complications (the virus can even nestle in the brain!) 29.4% of the British patients who got rid of SARS-CoV-2 were later readmitted in hospitals, and 12.3% eventually died, despite initially having survived the coronavirus!
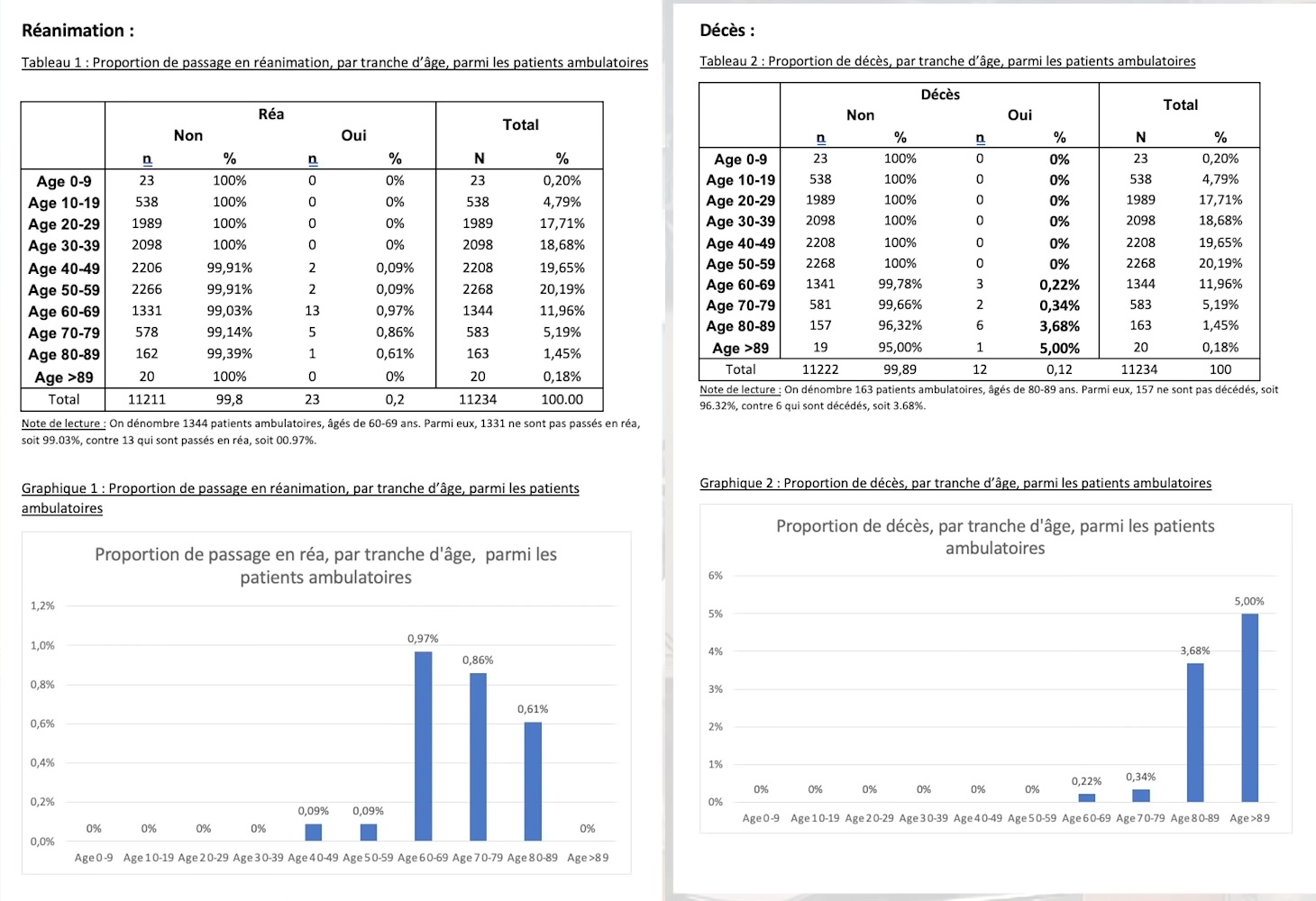
To confirm that Didier Raoult knows what he’s doing at IHU Méditerranée Infection Marseille, from IHU’s COVID outpatients, i.e. treated but not admitted to hospital:
- nobody died from the outpatients aged 0 to 59;
- overall, only 0.12% of the outpatients died (from 0.22% of those aged 60-69 to 5% of those aged 89+);
- nobody aged 0 to 39 needed intensive care;
- overall, only 0.2% needed intensive care.
One could conclude that, should everyone had been taken care of like at IHU Marseille, the huge problem of the ICU mechanical ventilators wouldn’t have existed!
Didier Raoult is also right to condemn France’s backwardness regarding RNA sequencing, even below many African countries (watch IHU’s video from Feb. 2, and the one from Jan. 19). But the same person expressed some questionable opinions:
- He insists that the importance of the face masks is relative (i.e. they should be used only by those known to be positive), and the most important is the hygiene (washing hands, alcohol). Well, OK, but how about the people who practically spit in one another’s face when talking or laughing?
- On Nov. 11, he reiterates that the hands are the major risk (because of what they touch: transmision manuportée des maladies réspiratoires), not the air that could carry the virus! 70% v/v alcohol is much more important than a mask! (Except for the caregivers, who are in close contact with the patients.) And that no, the second wave is not the fault of the French who did what they did in the summer holiday, but the borders should have been closed to the foreigners in tourist countries like France, Italy, Spain.
- On Jan. 5, he insisted that some other cheap medicines should be studied more with regard to COVID-189, namely ivermectin, cyclosporin, doxycycline.
- On Jan. 29, for Sud Radio, he insisted that no social measure had proven its effectiveness, being it lockdown, closing the bars and restaurants, etc. Starting from the fact that 55% of those infected were infected in their families, he concluded that most infections took place at home, not outside!
Now, Didier Raoult made the same mistake others did, and there are doctors, biologists, epidemiologists that fell for this fake logic; here’s the thing:
- Yes, keeping infected and non-infected people under the same roof eventually raised the infection rate, and not offering a proper treatment increased the death rate, BUT without a lockdown the sick people would have had the chance to spread the disease to many more people!
- The lockdowns were ineffective because they were “Western-style”: not true, but very partial lockdowns (and many people infringed the rules anyway). No matter what we think of China, only they had true lockdowns, with people never leaving their house, their block of flats or their neighborhood, or only being allowed to go shopping once a week; with people who were forced to sleep at the factory or at the power plant where they were working, without being able to return home for sleep and get infected in the process! China still actively traces the movements of everyone in the areas at risk–zero privacy, but fewer deaths. Take a look at this feature by ARTE, posted on Jan. 30, 2021 and online through Jan. 27, 2024: Chine : le retour du virus (also on YT); in English as China: Covid-19 is Back. Of possible interest too (but older), Chine, le paradoxe de Wuhan (also on YT); in English as China: The Wuhan Paradox (on YT too).
Everything that’s contagious and spreads when infected people contaminate objects touch by other people or infect other people directly through sneezing, coughing, laughing, talking can be diminished by reducing social contacts, FULL STOP.
As for the ivermectin I mentioned above, here’s a funny thing about it: there are close to zero chances for it to be proven effective, but there are groups of people strongly promoting it in some countries! (Note that on Feb. 4, 2021, Merck issued a statement on Ivermectin use, in which they explained how ivermectin simply cannot be of any use against COVID-19.) Now, some such people never believed in hydroxychloroquine, which however modulates the cytokine response, yet they praise the ivermectin! In my opinion, the fact that ivermectin inhibits the replication of SARS-CoV-2 in vitro doesn’t mean anything; Clorox kills the virus too, just not in vivo. Then, it’s known since May that the success attributed to ivermectin in some Latin American countries was partially due to a flawed database; also, the correlation-cum-causation ignored the fact that in areas where the population is massively carrying various tropical diseases, simply making those people free of such diseases through the use of ivermectin makes them more apt to react better to a SARS-CoV-2 infection! (It’s still possible though for ivermectin to have some effect on SARS-CoV-2, the same way people taking hydroxychloroquine for malaria had a better immune response to this coronavirus.)
Last but not least, there are idiots that keep being idiots, and the Chief Idiot seems to be Nicolás Maduro, who recently claimed to be in possession of the supreme COVID-19 killer, something called Carvacrol, which is…
“a thyme derivative with the chemical name of 2-methyl-5-(1-methylethyl)-phenol, and it’s nothing new, since both the extracts and the pure products of thyme already have a long tradition as nutritional and therapeutic agents since ancient times”. This is how the National Academy of Medicine of Venezuela defines Carvativir, the substance presented by Nicolás Maduro as the remedy against the coronavirus.
The Carvativir, Carvacrol or Cimofenol is a substance present in essential oils such as oregano and thyme, it has a yellowish or orange color, a spicy flavor, and a spicy smell like oregano. It can be used as a flavoring agent in food and different cosmetic products.
In addition, Carvatir is a very recurrent compound in homeopathic medicine, without any scientific basis, and is used in aromatic therapies to improve emotional well-being.
There are several scientific studies, such as the one carried out by the School of Chemical Engineering of the University of Yeungnam, in Korea, which assure that oregano oil, rich in Carvativir or Carvacrol, may have antibacterial properties. According to this study, this substance can help in the treatment of urinary tract infections caused mainly by the uropathogenic Escherichia coli bacteria.
It is not the first remedy against the coronavirus presented by Maduro. Last November, the Venezuelan president already assured that a group of scientists from the Venezuelan Institute for Scientific Research (IVIC) had found the cure against the coronavirus.
On that occasion, it was about another molecule, DR-10, that Rafael Lacava, a peculiar politician nicknamed Dracula, had extracted from an unidentified medicinal plant.
In addition, in March, shortly after the World Health Organization declared the coronavirus pandemic, Maduro already assured that Venezuela had a miraculous drug that was manufactured in Cuba, a kind of interferon. It didn’t take long for him to offer another remedy, this time homemade: a concoction of malojo, elderberry, ginger, black pepper, lemon and honey.
So it can be worse.
TWELVE
🟡 Back to the hydroxychloroquine, the “scientists” seem to never want to assess its effect on the disease or, in other terms, whether the chances of survival are better when hydroxychloroquine is taken prior to the infection, prior to the symptoms, or when the symptoms still don’t include a drop in the oxygen level in the blood. Here’s a study published online on Nov. 24, 2020, A cluster-randomized trial of hydroxychloroquine for prevention of COVID-19, who only assessed… the contagiosity!
Postexposure therapy with hydroxychloroquine did not prevent SARS-CoV-2 infection or symptomatic Covid-19 in healthy persons exposed to a PCR-positive case patient.
Here’s a study of this study, Understanding the drivers of transmission of SARS-CoV-2, published online on Feb. 2, 2021, which is totally useless IMO, but it includes this:
Although the effectiveness of masks is well established, in the analysis of Marks and colleagues, self-reported mask use surprisingly did not affect the risk of transmission. Similarly, Ng and colleagues did not find an effect of self-reported mask use on risk of COVID-19 transmission in their analysis of contact tracing data from Singapore. Rather than questioning the usefulness of mask-wearing policies, these results underscore the necessity of a multi-layered comprehensive approach to infection prevention and control. Factors such as consistent and correct use and quality of the mask could not be accounted for in the analysis.
Wow. We know they help, but they just didn’t. The masks. Correctly or incorrectly used. Not FFP2. Either way, the “well established” part is based on: Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis; and Effectiveness of face masks in preventing airborne transmission of SARS-CoV-2.
Self-reported things are tricky. “Oh, yes, I did use a surgical mask. But I didn’t wash hands that often, and I didn’t disinfect any objects, because I was wearing a mask, right?”
Good news though: remember how the French government forbade prescribing of the hydroxychloroquine for off-label uses, specifically SARS-CoV-2, and the town doctors (as opposed to hospital doctors) were revoked the right to prescribe hydroxychloroquine? Yes, in France, not in North Korea. It was on March 28 (chronology here). Well, Italy did the same on July 22, not by a Government Decree, but by the means of the Agenzia Italiana del Farmaco (AIFA). The good news for Italy came on Dec. 11, when il Consiglio di Stato, with Sentenza n. 7097/2020, nullified AIFA’s decision and reinstated the right to use the hydroxychloroquine for off-label cases, and specifically for SARS-CoV-2! (The full text also here, PDF versions here and here.) Not everyone is dictatorial on planet Earth!
As a result, the list of Farmaci utilizzabili per il trattamento della malattia COVID-19 now includes heparin, azithromycin, darunavir/cobicistat, lopinavir/ritonavir, hydroxychloroquine, remdesivir, corticosteroids.
THIRTEEN
🟡 Back to the lockdowns, so hated by some scientists across Europe. It has a small brother, the curfew.
I cannot help but express my astonishment that, while hundreds of thousands of idiots have demonstrated in most countries sometimes against lockdowns, sometimes against face masks (“Don’t muzzle us!”), they never demonstrated specifically against the curfews!
As it happens, the curfews are the only measure that is truly dictatorial. Lockdowns are dictated by the pandemic, and they weren’t true lockdowns à la chinoise. Face masks are a sanitary measure, and so is the disinfection. Social and physical distancing are also sanitary measures. But as long as one is allowed to get out of the house and go shopping for food in crowded supermarkets and using crowded streets, how can things improve by forbidding people to walk on empty streets in the evening or at night? This I will never understand, because there’s no logical explanation.
Official and officious explanations included mentions of people who prefer to break the law at night, when they get out to have a drink with friends on the street. Really?! In December and January, when it’s winter? And they’re fucking outside anyway, on empty streets! Change of mind: oh, but they might meet at someone’s house. Right, they only can do that after 8 PM or 9 PM, huh? But why can I just walk and get some air at an hour when the streets are empty, there’s less traffic, and the air is better? Just because I “might break the law”? By this logic, they should cut my dick off, because, you know, as long as I have such an organ I “might rape someone”!
Curfew only occurred during the war, in occupied territories. With low to nonexistent street lighting, the Résistance was likely to prepare sabotages, so any patrol, being they the Wehrmacht, the SS, or the Gestapo, could have shot anyone on sight. But are we in such a situation?
Not only the deniers failed to demonstrate against curfews, but those who said “there’s no study to prove that lockdowns/distancing/masks/etc. have any effect” also failed to react to the lockdowns!
The funniest and the most grotesque thing is what happened in France: initially limited to some areas, since Jan. 16, a curfew starting at 6 PM is in place on the entire territory of France! Mind you, it was exactly between 6 PM and 8 PM that the virus was spreading the most! Not after 8 PM or 9 PM, but since 6 PM onwards.
Based on the official reports, this extension of the curfew had some results in curbing the contagion. But it’s exactly because at 6 PM you cannot call it a curfew. Say you forbid people to be on the streets and in shops past 4 PM. Make it 2 PM then. This is not a curfew, but a partial lockdown, and this is why it (kind of) works! Actually, they could have imposed a lockdown during the day and freedom of movement during the night, when no shop is open, and the results would have been even better!
But France has one of the most inept governments in Europe…
FOURTEEN
🟡 Zero-COVID as a policy. I’ve always said that what happens now in the West is the result of a “fake lockdown”; it’s only recently that I became aware that reason exists in the Western world too, and some people have created the Zero Covid initiative in the UK. Here’s a summary of a Zero-COVID strategy, and here’s an excerpt from the German site CARTA, written by Prof. Yaneer Bar-Yam, the founder of EndCoronavirus.org:
But even Germany, once considered within Europe as a model for its COVID-19 response, has not fared well in comparison to many Asia/Pacific countries that opted for a »Zero Covid« strategy.
Thailand, for example, has a population of 69 million, but has only suffered about 60 deaths from COVID-19 since the start of the pandemic. Meanwhile, Germany — population 83 million — has had more than 26,000 deaths. What’s more, Germany is currently locked down, while life in Thailand is close to normal.
Residents of New Zealand, Australia, Taiwan, and Vietnam, are also enjoying something very close to normal life because their governments made the right decisions: they chose a »Zero Covid« strategy. This, even with the need to respond to occasional small outbreaks.
… Since March, it has become clear what elements are key to a successful Zero Covid strategy. I would like to highlight six lessons from the Asia/Pacific success stories that should be applied everywhere:
1. Target zero cases and treat every single new infection as a national security threat. (In contrast, in the United States and Europe, authorities aim to keep COVID-19 cases at a »manageable level.« Unfortunately, a permanent »soft lockdown« is required to keep the »manageable« level of transmission of cases from exploding into exponential growth, and no country has been able to stomach a permanent soft lockdown.)
2. When community transmission first appears, impose short, strict lockdowns – combined with masks, tracing, and ventilation – to get to zero cases. (In contrast, in the United States and Europe, authorities often wait to impose restrictive measures until hospitals approach full capacity, and then often only impose »soft lockdowns.«)
3. Isolate infected individuals and their contacts in »quarantine hotels« or specialized facilities. (In contrast, in the United States and Europe, authorities advise infected individuals and their contacts to self-quarantine at home. These individuals then infect their cohabitants or violate quarantine and infect others.)
4. Prevent importation of new cases through mandatory quarantines on travelers from »red zones.« (In contrast, in the United States and Europe, most travelers from places with active transmission can avoid mandatory quarantine if they provide a negative PCR test, which has a high false negative rate. And »mandatory quarantine requirements« are typically not strictly enforced.)
5. Sub-national regions reopen through »green zone« strategy, in which COVID-free »green« zones reopen while restricting travel from »red zones.« (In contrast, in the United States and Europe, regions reopen before transmission is eliminated. When »green zone« status is achieved in sub-national regions, authorities do not protect these through travel restrictions.)
Many of those in Europe and the United States who accept that getting to zero Covid is possible claim that it could not work in the West because it »too costly«. However, when community transmission is taking place, the set of actions required to prevent exponential transmission growth is both costly and neverending. Without economically prohibitive measures, another Covid wave is guaranteed to occur, requiring yet greater costs to suppress, as well as the additional loss of health and life.
The larger the number of cases per day, the more costly it is to contain the virus. Why would any country not invest in the short term to reduce new cases to as low a number as possible? Then they could control the virus with fewer social, economic, and health costs for the remainder of the pandemic. Why not get to zero community transmission, so that the economy can truly open up again?
The MIT Professor forgot to mention that the idiotic way this pandemic was handled in the West is rooted in the inept vision of “freedom is more important than public safety and national security,” to the extent that people had to die of COVID-19 for the sake of an illusory “freedom.”
FIFTEEN
🟡 What’s going to happen next? Are we going to have enough vaccines to reach “herd immunity” by the end of this year? (Rather unlikely.) How about the poorer countries that, even in Europe, still lack a vaccine? And how can the EU impose “vaccination passports” as long as there’s a shortage of vaccines? (The case of an “immunity passport” has been discussed while in the first wave, but the EU is considering it only now.)
We might need COVID-19 vaccines for many years to come, says Angela Merkel. Is then the pandemic really going to last 4-5 years? How dangerous is the new E484K additional mutation adopted by variants of the British B.1.1.7 variant? What if each new wave is like a new pandemic, and the vaccines are only half-effective? Note that AstraZeneca’s vaccine (AZD1222 aka ChAdOx1, also manufactured by Serum Institute of India as Covishield) is the one with the bizarre behavior that makes it untrustworthy: its efficacy is 62.1% for two standard doses, but 90.0% for a low dose followed by a standard dose; now they put it at 82% after a second dose, which is rather low. Novavax (NVX-CoV2373) is also questionable, with 89.3% efficacy in the UK (B.1.1.7 and other variants), but only 60% in South Africa (B.1.351 variant). Is the South African variant the one that will kill us? (We might need to use better face masks.)
Are new treatments going to surface, beyond the aforementioned REGN-COV2 and XAV-19? On the cytokine-modulators side, there’s the new EXO-CD24 (New Israeli drug cured 29 of 30 moderate/serious COVID cases in days; the 30th patient also eventually recovered), but Big Pharma might conspire against it; here’s a German article mentioning it that ends this way (automated translation):
Still little reason for euphoria
This is not the first time that news of success like this has gone viral. Pharmacologist Michael Freissmuth from MedUni Vienna is correspondingly critical. Because: “With only 30 patients observed, one can at best say: nice observation,” says the expert. As long as there are no clinical studies, no insight into the data and no control groups, one cannot assess an effect with regard to the different courses of Sars-CoV-2.
Freissmuth therefore calls the advance of the physicians “a media rapid-fire reaction.” Because the difficult thing about Covid-19 courses is that “after the administration of some drugs, you can say that isolated patients get better, but there are no control groups to prove it.”
He therefore appealed to responsible scientists and physicians not to “rush out” such findings, but first to “back them up with clinical data.” Because the majority of anecdotes still do not make evidence, he says. And evidence is “pretty clearly settled” in medicine, he adds.
What is pretty clear in medicine is that bureaucracy and cupidity killed too many people in this pandemic. Should EXO-CD24 have the fate of hydroxychloroquine… we’ll be proven stupid as a species.
SIXTEEN
🟡 Finally, is the economy going to survive? Take a look at what’s left of Los Angeles! (But maybe we should be confident that Homo sapiens americanus won’t become extinct, despite not being able to name a single country on the map.)
People want their old life back, but the post-COVID world is impossible to predict, so I won’t speculate on anything. What I don’t want to need to write again about, is pandemic.
In the event that I am reincarnated, I would like to return as a deadly virus, to contribute something to solving overpopulation.
— Prince Philip, the Queen’s consort, in 1988
LATE EDIT—BONUS
🟡 I forgot to mention our friends the Italians. In the section “smart people telling stupid things” (ELEVEN), I didn’t mention how much I keep being disappointed by Enzo Pennetta, a very intelligent biologist (and controversial at that, which is a sign he troubles the waters of the mainstream dogmas). You’ll find him on the blog Critica Scientifica; he used to be invited in Claudio Messora’s ByoBlu videos, but in recent times he too has a YT channel. Now, the problem with Professor Pennetta that he continues into the trend of those saying that everything that is done is wrong, dictatorial, with financial interests, and, of course, that this is not a pandemic when only 0.3% of those infected die. He’s not entirely wrong, but his attitude doesn’t create a “healthy doubt” (as Éric Zemmour would have said), but rather “unconstructive criticism.” Even less constructive than Enzo Pennetta is Claudio Mesora’s other guests and the ideas selected to be disseminated via ByoBlu, including among the most innocuous of them the famous “This virus has not even been isolated: it is a nucleic acid sequence invented in a computer lab, which repeats the structure of the first SARS-CoV.”
Much more honest is the criticism presented by Sigfrido Ranucci in Rai’s weekly Report investigative series. I’ll now comment on the Jan. 21, 2021 episode, more precisely on the segment Nelle mani del vaccino (Manuele Bonaccorsi, Lorenzo Vendemiale), which is approximately between the minutes 41 and 70.
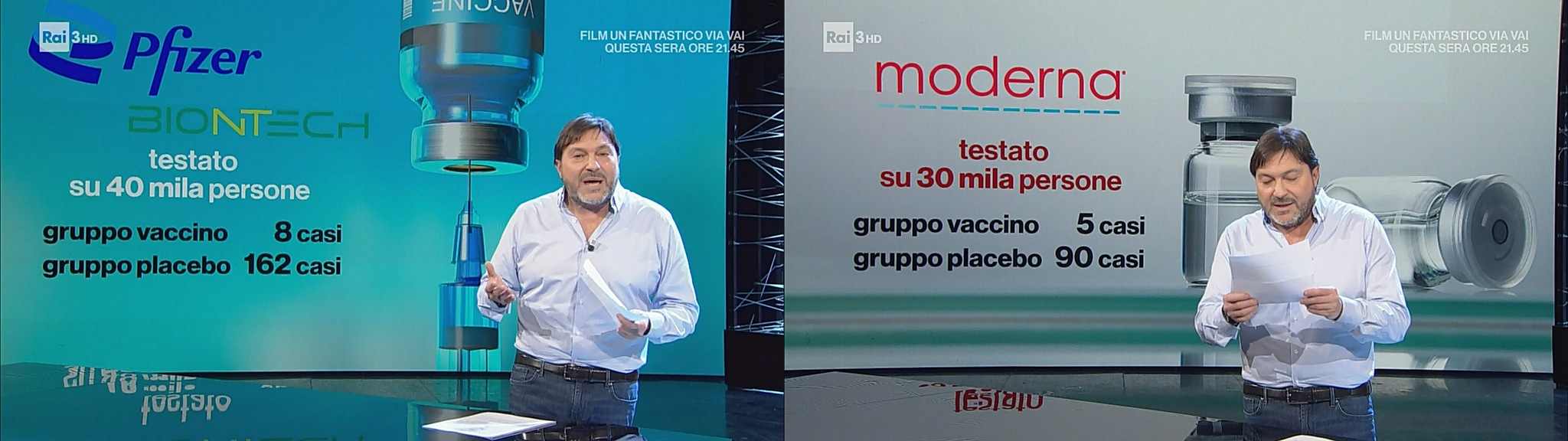
The efficacy of the first vaccines to be approved was based on a moderate number of trial participants (see the screenshots above), which apparently led to very few cases of “lack of efficacy.” But how was this determined?
First, we discover that most trial voluntaries for Pfizer and Moderna were never tested more than once–the day before the vaccination (with the vaccine or with a placebo); a German doctor confirms: the parameters of this study were established by Pfizer.

Prof. Peter Doshi, University of Maryland: The 95% efficacy of the vaccine is referring to a very specific aspect: the decrease in the symptomatic cases, not a 95% reduction of the infection rate! The trials were not conceived to reveal that.
Prof. Andrea Crisanti, Università di Padova: Even vaccinated, one may pass the virus to others. This is confirmed by Dr. Nicola Magrini, head of AIFA (the Italian Medicines Agency): even if everyone is vaccinated, the herd immunity and stopping of the coronavirus spreading are “not automatic.”

Prof. Peter Doshi: There were two options the pharma companies were facing: to prove a reduction in the infection rate, or to prove a reduction of the sickness rate. They have chosen the second one.
This is not necessarily evil per se. A vaccine’s first task is to prevent the death or the severe incapacitation of those vaccinated; stopping the epidemic (or pandemic) is only a by-product. But here the stakes were higher.
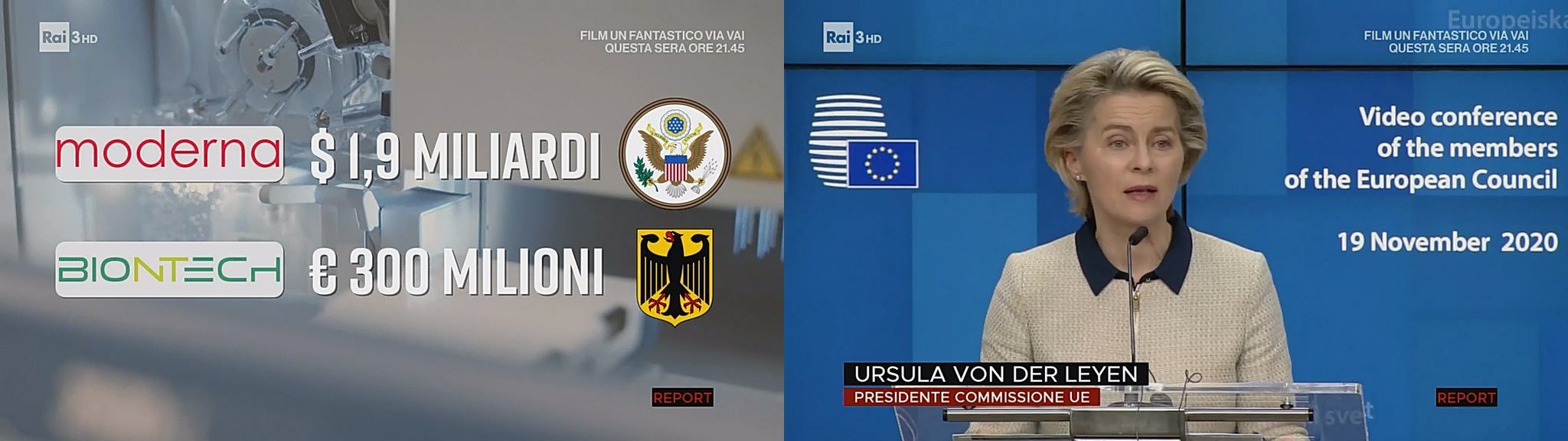
The two major Pharma companies were given huge subsidies from the US (for Moderna) and from Germany (for BioNTech). There was zero transparency as to how the money was used, and yet, on Nov. 19, Ursula von der Leyen announced that the vaccines will soon be approved–although the EMA insists that they’re independent of the European Commission.
As it was the case, there were serious doubts that the vaccines were ready for the market, but from now on I’ll refer to the original sources, not to Rai’s Report.
Before getting to quote from the Flemish NGO Journalismfund.eu, who covered the topic Behind The Pledge – How EU money is spent for Covid19 drugs, let’s take a detour to visit the British Medical Journal, where Prof. Peter Doshi harshly criticized the Big Pharma: Will covid-19 vaccines save lives? Current trials aren’t designed to tell us.
The world has bet the farm on vaccines as the solution to the pandemic, but the trials are not focused on answering the questions many might assume they are.
…
But what will it mean exactly when a vaccine is declared “effective”? To the public this seems fairly obvious. “The primary goal of a covid-19 vaccine is to keep people from getting very sick and dying,” a National Public Radio broadcast said bluntly.Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”
Yet the current phase III trials are not actually set up to prove either. None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
…
In a September interview Medscape editor in chief Eric Topol pondered what counts as a recorded “event” in the vaccine trials. “We’re not talking about just a PCR [polymerase chain reaction test]-positive mild infection. It has to be moderate to severe illness to qualify as an event, correct?” he asked.“That’s right,” concurred his guest, Paul Offit, a vaccinologist who sits on the FDA advisory committee that may ultimately recommend the vaccines for licence or emergency use authorisation.
…
“Our trial will not demonstrate prevention of transmission,” Zaks said, “because in order to do that you have to swab people twice a week for very long periods, and that becomes operationally untenable.”
…
Zaks added, “A 30 000 [participant] trial is already a fairly large trial. If you’re asking for a 300 000 trial then you need to talk to the people who are paying for it, because now you’re talking about not a $500m to $1bn trial, you’re talking about something 10 times the size.”
As previously said, they didn’t assess the ability of vaccination to stop the transmission, for it would have been “untenable” and too expensive. And an “event” or a failure of the vaccine was only a moderate to severe illness! Was the public made aware of this?
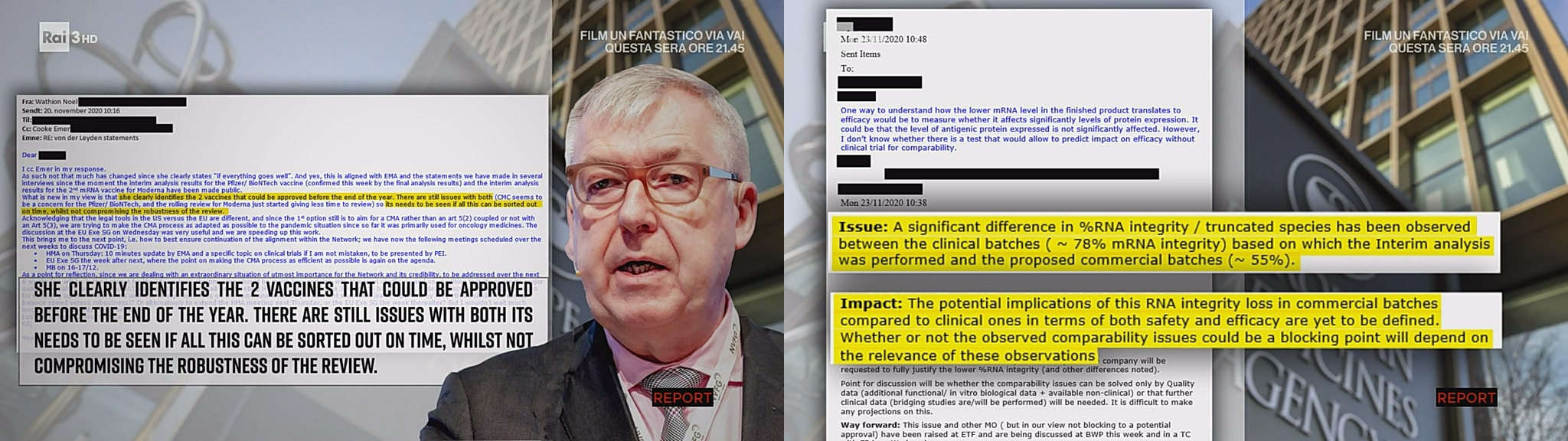
Back to the documents cited by the Rai investigation, via Journalismfund.eu:
- From the EMA internal e-mails found on the Dark Web: regarding Pfizer/BioNTech, the mRNA integrity in the commercial vaccines is inferior to those used in trials, on average 55% vs 78%.
- From another document, the mRNA for clinical trials was 69-81%, while for the commercial batches was 59% on average, but as low as 51-52%, was saying the EMA on Nov. 23. (And when you think that the manufacturer agreed that using a 5-dose bottle to vaccinate 6 persons is OK! Let’s dilute furthermore something that’s already too diluted!)
- The contracts between the European Commission and the vaccine manufacturers were secret, and only after the Corporate European Observatory has filed a complaint with the European Ombudsman, the EU agreed to disclose the contracts with Curevac and AstraZeneca, but the key elements were redacted (censored).
This shouldn’t be a reason for us to refuse the vaccine. After all, the Israelis, who have vaccinated and tested millions, reported that just 0.04% of Israelis caught COVID-19 after two shots of Pfizer vaccine.
What we should do when all of this is over is to dismantle this nest of rats that is the European Union corrupt bureaucracy and return to a Europe of nations, with bilateral and multilateral agreements on the movement of persons, goods, and capitals! The USSR fell apart, and the only similar construct is the EU.
We must survive, but the EU should die!
AN EVEN LATER EDIT
🟡 Maybe we should dismantle all the political, scientific, and other kinds of authorities that lost all their credibility in this pandemic. Here’s a recent one:
- Remember how authorities in several countries (Germany, Austria, Sweden, Norway, Denmark, Netherlands, Spain, Poland) said AstraZeneca’s vaccine might not be effective over 65 years of age, for lack of data? L’idiot suprême, Emmanuel Macron, said AstraZeneca’s vaccine “is quasi-ineffective” for people over 65. Italy and Belgium even set 55 years for an age limit, and Switzerland refused to approve the vaccine altogether.
- The UK disagreed and approved it for all ages, and some other countries did the same (India, Mexico, Argentina).
- On Feb. 10, the Strategic Advisory Group of Experts (SAGE), an advisory group to the World Health Organization, announced at a press conference that it has recommended the AstraZeneca vaccine for adults 65 years old and older, “based on their review of a more limited set of data in conjunction with data from all age groups” and given that “we feel that the response of this group cannot be any different from groups of a younger age.”
- Angela Merkel went gaga and said, on Feb. 25, that she’s “at 66 too old for this vaccine,” but otherwise “it’s a good, safe and effective vaccine.” Fucking shit! How would the German people trust this vaccine? Obviously, there’s no sharp age barrier at 65, but seeing their Chancellor refusing the Oxford/AstraZeneca jab for a mere one year more of age, people might start asking themselves: “hey, maybe it’s risky to have it even at 64 or 63!” UPDATE: On March 4, the German Vaccine Commission (Stiko) decided to recommend this vaccine even for people over 65, effectively making the German Chancellor a laughingstock (she could and should have said “I’m still waiting for our experts to decide whether it’s advisable for my age”).
- Actually, a Guardian investigation found that 4.85M of the 6.13M Oxford/AstraZeneca doses distributed throughout the EU haven’t been administered, most likely for these reasons: an “acceptance problem”; the artificial age limit of 65; the inability of those stupid governments to simultaneously focus on both older people (for which other brands are preferred) and younger people (for which this jab is mostly fine, even if not the most effective one). So if ~80% of this jab was still unused, 80%+ of the supplied Pfizer/BionTech doses were already administered in countries such as Belgium, Italy, Germany.
- Still, the mainstream media relies to propaganda. Euronews: Angela Merkel did not “refuse” the AstraZeneca vaccine, despite this being reported. Of course she did refuse it, even if it was because of her age! Instead of saying she refused it for other reasons than efficacy, they preferred to act like Goebbels! Another propaganda message: “Don’t believe the fake news; AstraZeneca is very good and effective!” Oh, so all those studies suggesting it offers as little as 10% protection against the South African variant are fake news?!
Wonderful. One more of these:
- South Africa halted its AstraZeneca vaccine rollout due to its low efficiency against the B.1.351 variant and said it would be using the Johnson & Johnson vaccine instead.
- Only days later, in Romania, people flocked to be vaccinated with AstraZeneca’s jab: 200,000 vaccination slots got booked in about 10 hours.
AstraZeneca über alles!
A last idiocy from the kingdom of Emmanuel Macron: France’s Haute Autorité de Santé recommended on Feb. 12 only one dose of the vaccine to people who have previously contracted COVID-19. This single dose of vaccine would act as a booster (second dose, rappel) for such people. The only studies that support this decision: one on 109 people (of which 41 had previously tested positive); another one (not peer-reviewed!) on 59 people. This is preposterous and, given the size of the studies, they’re almost “anecdotal evidence”–the usual epithet such authorities use to reject anything that doesn’t serve their interests. But here, there is obviously an attempt to save money and to be able to report a successful mass vaccination in a country where almost everything goes wrong… Heads have fallen for less than that, but Emperor Macron is insouciant.
The epilogue is still to be determined…
NINETEEN
🟡 Speaking of credibility and trustworthiness, whatever was left of them just went down the drain. Let’s talk of the greed that motivates Pfizer/BioNTech:
- They played poker in Peru: for 20M doses (if ever), Pfizer wanted government property as collaterals in case the country can’t pay for the vaccine. Negotiating a life-saving vaccine in a global emergency under such terms and conditions is beyond immorality. And the talks are fully confidential, including whatever contracts are signed–the same as the contract between Pfizer and the EU. Obviously, transparency would mean they couldn’t fuck Peru as they intend to!
- The rest of Latin America is not spared either. While Chile has negotiated early and now is able to vaccinate, countries like Colombia, Costa Rica, the Dominican Republic, Ecuador, Mexico, Panama, Peru, Uruguay, Argentina and Brazil are bullied by Pfizer. Only the last two have ordered their vaccines from Russia, after having been asked impossible conditions. Argentina has been asked to assume whole responsibility if Pfizer… fails to deliver or if it delivers a defective vaccine, and Pfizer asked for collaterals including embassy buildings and military bases! Similar conditions were imposed to Brazil.
- The Bureau of Investigative Journalism has more: ‘Held to ransom’: Pfizer demands governments gamble with state assets to secure vaccine deal.
Meanwhile, as we discover there’s an even newer UK variant (B.1.525), and a new NYC variant (B.1.526), everyone is trying to sell their vaccines, effective or not.
- AstraZeneca is known to be not only the cheapest but also possibly the least effective against the South African variant–but who cares? This jab made health workers in France, Germany, Sweden suffer side-effects (in Sweden, two of 21 healthcare regions paused vaccinations of workers last week after a quarter called in sick after getting the AstraZeneca shot), but hey, everything is normal according to the best experts!
- Pfizer claims their vaccine is so effective that’s actually too effective: an efficacy of 92.6% after the first dose is claimed (compare to 92.1% reported for Moderna). And yet, while they say the second dose can be delayed thanks to the efficacy of the initial one, they also test a third dose to boost the effect even more–or is it merely to be able to sell more? “We believe that the third dose will raise the antibody response 10- to 20- fold.” (¡Madre de Dios!)
- In UK, the morons are planning to schedule the second dose 12 weeks after the first one, despite no clinical evidence to prove it’s effective this way.
- On the other hand, Pfizer now claims there’s no need to store the vaccine at -70°C, but -25°C to -15°C is just fine for two weeks.
- Johnson & Johnson‘s vaccine will soon be approved in the US, and Dr. Fauci warns against cherry-picking, urging people to take whatever brand is available. But Johnson & Johnson vaccine’s efficacy was just 57% in South Africa, where B.1.351 is now the dominant variant, compared to 72% in the US, where it is far less common. And even 72% is not the greatest figure yet.
But the entire process of preordering these vaccines is flawed. The EU Commission doesn’t know which other venues there are for other countries to get vaccines from those major pharma companies, and indeed there are negotiations with individual countries even here in Europe. The COVAX initiative is a big flop, so it’s no wonder that Hungary now also uses both the Russian and a Chinese vaccine, or that San Marino (this small anomaly of a state is not an EU member!) also had to resort to the Russians!
But why hasn’t the EU approved the Russian Sputnik V vaccine? It’s all politics, or the New Cold War, if you prefer. It’s not worse than AstraZeneca’s almost useless jab (IMO), and its adverse reactions, while often including flu-like fever, are quite similar to AstraZeneca’s! So I suppose all the smart guys should rather go for Sputnik V… and possibly for the Chinese vaccines too. The Hungarians came with an extremely sensible principle: A government decree streamlined Hungary’s vaccine approval process by allowing any vaccine administered to at least 1 million people worldwide to be used without undergoing review by the country’s medicines regulator. Voilà.
Or maybe all vaccines should be “nationalized” in the sense that, patented or not, they should be declared free to manufacture and use, no royalties whatsoever! The idea is not new, according to Le Monde: Napoléon Ier, les vaccins et la propriété privée : « Si ce remède [produit] des effets utiles à l’humanité, le secret sera publié sans délai ». After the imperial decree signed by Napoleon I in 1810, and the law of 1844, “pharmaceutical compositions and remedies of any kind” were excluded from patentability, so that Pasteur could not patent any vaccine (but he could patent the pasteurization). It was only in 1968 that pharmaceutical products were reinstated in France under the ordinary patent law, but with a “compulsory license” clause for public health reasons (insufficient production, abnormal prices). Maybe it’s time to so do something of the kind regarding the SARS-CoV-2 vaccines, but under whose leadership? The UN, the WHO, the EU, NATO? They’re all laughingstocks.
An Italian newspaper gives a nuanced answer to the question Without patents, would we have more doses of vaccines?, and it’s not an optimistic one. Of course, Resolution 58.5 of the World Health Assembly, the legislative body of the World Health Organization, provides that during a pandemic, governments can implement all the necessary measures to improve the supply of medicines and vaccines, “using to the full the flexibilities contained in the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS),” the standard for the management of the intellectual property in the international context. As per Article 31 of TRIPS, a government could even establish a compulsory license, that is, to be able to use the patent even without the consent of the person who registered it. Producing coronavirus vaccines independently and without the consent of the pharmaceutical companies that developed them isn’t that simple though, because what most pharmaceutical companies can do is the “fill and finish” phase, which is much more than just filling vials, but doesn’t include the production of the “active ingredient.” Nonetheless, Novartis said they’re ready to produce such vaccines in Italy, if allowed to.
Riccardo Ruggeri insists that Big Pharma might want out of the vaccine industry for not being profitable enough, and low prices (as wanted by the EU), combined with the risk of nationalization of the patents, can’t do any good. (Also, long-term investments aren’t what the shareholders want to hear about; still, Israel managed to purchased vaccines more expensive than the market price.) In the meantime, Italy decided to manufacture the Russian Sputnik V vaccine.
TWENTY
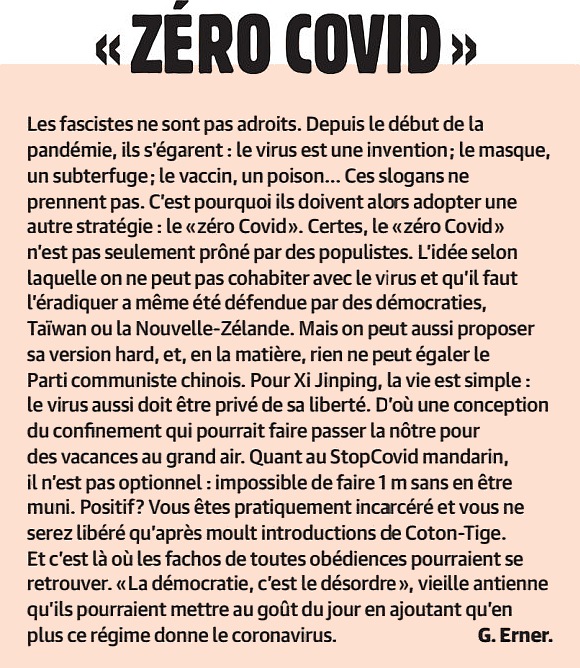
🟡 “Back to Normal” is going to be extremely questionable. In section FOURTEEN, I mentioned the “Zero COVID” policy. Here’s Guillaume Erner, in Charlie Hebdo of Feb. 17, 2021, comparing it to fascism (more precisely, to Chinese fascism):
Needless to say–I always make it clear–the world is full of idiots. Without such idiots, there would be no need to impose a truly fascist 6 PM to 6 AM curfew in Alpes-Maritimes because those fucking morons wouldn’t have reached the incidence rate of 600 in 100,000! Without such idiots, the Czech Republic wouldn’t be as high as 915 in 100,000, but this happened because 47% of Czechs admitted to not staying at home even if they suffered from COVID-19 symptoms, 76% do not trust the government’s messaging about the pandemic and 45% believe the risks are exaggerated by the media or politicians.
This is the world we’re living in. Of course, the authorities aren’t much smarter either. There is no logic and no consistency whatsoever in their restrictions. Take the small towns of Ulm (Baden-Württemberg) and New-Ulm (Bavaria), less than 2 km away on foot and 5 km by car. From March 1, hardware stores are opening in New-Ulm, but not in Ulm, as the two neighboring German States have different regulations. In the first lockdown, it was the other way around! Then, an Administrative Court ruled that driving schools in Baden-Württemberg, which were closed by State regulations, must open from March 1 when the minimum distance between the driver and the instructor can be maintained, e.g. for bus and truck drivers. It’s really embarrassing to govern through courts of law! And a last one from BW: hairdressers and garden shops can open, but not the other “non-essential” stores such as those selling clothing or electronics! WARUM?!
To be honest, the virus can spread much easier in supermarkets and discounters than in other kinds of stores. The current restrictions only harm the economy, and they’re downright murderous at times: I’ve read of suicides in many countries, all “thanks to” this pandemic, and to its mishandling.
To be even more honest, if most people had common sense and decency, there wouldn’t have been any pandemic at all. I still don’t get how the disease managed to spread that fast everywhere, and it still spreads here and there at an appalling rate–it’s like rabid rabbits with AIDS were fucking 24/7, and even then the result wouldn’t be an AIDS pandemic!
- If only people had worn a face mask even for the common flu, the way they do it in some Asian countries…
- If only people stayed at home when feeling sick because, at least in Europe, paid medical leave is easily available, unlike in America…
- If only people kept a decent distance between them at all times instead of behaving like canned sardines or worms…
- If only people gave up some stupid national habits such as cheek kissing when meeting (the norm in France and Italy)…
- If only people stopped talking too loud and literally spitting while doing so, or laughing like fools also with emanations of droplets, all this while being way too close to other people…
- If only people had the instinct of hygiene and cleanliness and washed their hands after having touched door handles, merchandise in stores, and any other potential sources of bacteria and viruses…
- If only people limited their air traveling to real emergencies instead of going around the globe like fools just because they could… (Not just the airports per se, but those horrendous COBUS airport buses are probably the source of most infections, knowing that they’re always packed!)
- If only people weren’t so stupid!
But here we are, sabotaging ourselves as a civilization. It’s no wonder several anti-COVID-measures political parties have been created! In Germany, dieBasis and WiR2020. The wrong answer (worse than what’s commonly called “populism”) to a true problem (true democracy doesn’t exist anywhere).
Apparently, SARS-CoV-2 is here to stay. Beyond the improperly called “long Covid” (why not “long-term Covid”? Dr. Fauci invented for it the term PASC, which sounds like shit), it looks like this virus is likely to remain endemic in populations at least for several years, possibly indefinitely. A study published in the peer-reviewed journal Science found that the virus “could join the ranks of mild, cold-causing … human coronaviruses in the long run.” SARS-CoV-2 might eventually be no more virulent than the common cold, but we have to reach that phase first. Also,
On the other hand, accepting endemicity means we will have to “tolerate” some level of deaths, probably with seasonal peaks. This is how we currently handle seasonal influenza; we work to minimize infections and their consequences when we cannot eliminate them, and society accepts the resulting risks. Risks cannot be reduced to zero or none of us would ever get in a car.
But then, we might “invent” another genocidal virus, argues John Oliver in “The Next Pandemic“:
The proof that we didn’t learn anything from this pandemic: Opening the windows against Covid-19 is very important, but if no one talks about it anymore. Ventilating rooms remains a very effective way to protect yourself from any respiratory disease. Automated translation from the Italian edition of Esquire online:
During the first lockdown, there was a lot of talk about this method, but it was aimed above all at the management system of workplaces, offices, shops, etc., but now that the pandemic continues it is increasingly clear that this habit must be extended to everyone.
Especially now that we are going through the last months of cold and that we tend to keep the rooms warm, this aspect of safety for oneself and for the people with whom one lives should not be forgotten. SAGE (Scientific Advisory Group for Emergencies) reopened the discussion with important statements: “Clear messages and guidelines will be needed to improve understanding of why good ventilation is important and how to effectively use ventilation systems or achieve good natural ventilation.”
This November, the British government launched a campaign with very clear directions in this regard: open windows fully for 10-15 minutes regularly during the day or leave them open all the time. This reduces the risk of particle infection by more than 70%. Yet according to polls, too few people have made this a habit. In Japan, the government advised people to open their windows at home for a few minutes twice an hour.
Yet this story of open windows is nothing new, indeed it has been part of our “medical culture” for many years. In the second half of the 18th century, there was a growing concern about air in confined spaces causing disease. In his 1769 book Domestic Medicine and the Family Physician, Scottish physician and writer William Buchan noted that for many people, “low, dirty homes are the places where contagious diseases lurk.” In 1842, a contributor to the Report on the Sanitary Condition of the Laboring Population of Great Britain reported that when many people are crammed into relatively small spaces and ventilation is neglected, it is possible for a fever to originate with great ease.
In her 1859 book Notes on Nursing, Florence Nightingale emphasized the importance of open windows in the fight against disease. “Cleanliness and fresh air from open windows with relentless attention to the patient are the only defense a real nurse asks or needs,” she wrote.
In hospitals, the use of open windows to improve ventilation was used on victims during World War I and during the 1918-1919 flu pandemic, when patient beds were even placed outside.
The examples would be many, but the concept at the center remains clear. Whether it’s winter or summer, in cases like those we are experiencing an open window becomes a precious asset. Let’s not forget it.
The Atlantic has a much more elaborated story, We’re Just Rediscovering a 19th-Century Pandemic Strategy. Yes, it originated in the “miasma theory” (i.e. the disease originates from “bad air”) back from when germs were unknown, but it’s still valid today:
This idea peaked in the 19th century, when doctors, architects, and one particularly influential nurse, Florence Nightingale, became fixated on ventilation’s importance for health. It manifested in the physical layout of buildings: windows, many of them, but also towers erected for the sole purpose of ventilation and elaborate ductwork to move contaminated air outdoors. Historic buildings still bear the vestigial mark of these public-health strategies, long after the scientific thinking has moved on.
The obsession with ventilation—and miasma theory in general—was indeed wrong when it came to pathogens such as cholera and yellow fever that we now know spread through other means (water and mosquitoes, respectively). But it did make sense for the diseases that invisibly stalked people through 19th-century air: measles, tuberculosis, smallpox, influenza—all much diminished as threats in the 21st century. “We’ve gotten so good at preventing so many diseases, there’s been a loss of knowledge and a loss of experience,” Jeanne Kisacky, the author of Rise of the Modern Hospital, says. Science is not a simple linear march toward progress; it also forgets.
…
Homes needed ventilation as well. In Victorian England, reformers successfully fought a window tax that penalized large windows, says Henrik Schoenefeldt, an architectural historian at the University of Kent. Bigger windows meant better ventilation. One doctor, Schoenefeldt told me, even railed against small windows as a “crime” that was killing people.
…
Stupidity is killing people. Amen.
As of week 2021-7, over 530,000 Covid-related deaths have been reported in the EEA (population 540M), and over 500,000 in the US (population 330M); in the case of the US, this tops the number of Americans killed in World War II (405,000), Korea (36,000) and Vietnam (58,000) combined.
I, for one, believe a new wave’s going to have disastrous consequences in Europe and in North America after the summer holidays.
TWENTY-ONE
🟡 More than one year since it all started, we’re worse than in Idiocracy. Here’s a few more proofs:
- The Czech Republic currently has the highest rate of new infections in the entire world, with (as of March 5) the 7-day incidence per 100,000 inhabitants of 805 (compare to 68 for Germany, 126 for the USA, 191 for Brazil). Whatever they do, they’ve just proved to have a negative IQ.
- While in Texas the infection rate is rising, and they have discovered all the “new” variants of interest (British, South African, Brazilian), the Governor decided to lift the mask-wearing requirement and to “open Texas 100%”! Yeah, the same state unable to adapt the Building Code to a changing climate, the same state unwilling to connect its power grid to the neighbors, the state of the brainless. NOTE: the “opening” of Texas means that wearing a mask was not mandated anymore by any law, regulation, or executive order, but businesses were still free to impose wearing of face masks on their premises; this wasn’t easy though.
- Even worse, the US Supreme Court blocked a ban on church services in Santa Clara County, California, without even bothering to explain why! As the article explains, “its underlying message is relatively clear: Religious exercise now gets special benefits above and beyond all other First Amendment activities. Why? We don’t really know.” Simply put, who cares about COVID-19 and public health, going to the church comes first in America! (One more proof that the SCOTUS is not a court of judges, but a court of politically appointed persons that happen to be judges, and that also happen to be stupid bigots.)
TWENTY-TWO
🟡 Two unexpected bad news this March. The first one: several countries where the vaccination figures are rather good, from Brazil to Serbia (later Hungary), have huge spikes in the severe COVID-19 cases. Of course, Bolsonaro always downplayed the issue (and he’s still doing it), and Serbia had a poor record handling this pandemic too, but I think the explanation is elsewhere. (No, not that some of the vaccines they used were Chinese or Russian.) I’d say that people got too happy too soon. You really need to have vaccinated more than 70% of the population to start feeling secure! But this “COVID fatigue” made people let down their guard too soon. They want it all to end now, but the virus couldn’t care less of what people want.
And then, this stupid temporary suspension of two batches of the AstraZeneca vaccine, ABV2856 and ABV5300, in at least nine European countries, for reported blood coagulation issues, including the death of a few people (at least one in Italy, one in Austria, and a couple of other suspicious deaths). The problem is not the suspension of the vaccination per se, but the way they handled the “de-demonisation” campaign! By “they” I mean the politicians, from Ursula VDL to Mario Draghi and other top European politicians; I mean the national health care “gurus”; and I mean the European Medicines Agency.
What they did:
- “there’s no proven connection between the jabs and the deaths”
- “the number of adverse reactions are statistically consistent with the adverse reactions to other vaccines too, including e.g. the flu vaccine”
- “we have studied the data and there’s nothing wrong with these batches”
- “this is a safe, approved vaccine”
- “the benefits of AstraZeneca outweigh the side effects”
What they should have done:
- They should have stopped reading the bloody certification papers and start analyzing the manufacturing and bottling process!
- They should have identified the possibilities of having defective vials, and the granularity of the process: can a single vial have spurious substances, an incorrect amount of the viral load, etc., or an entire batch must be defective in such a case? Remember how sometimes entire batches of shampoo, baby food, mustard, meat products, etc. etc. are recalled, but for that to happen one need to identify both (1) the cause of the non-conformity, and (2) the manufacturing period and place, with as fine a granularity as possible!
- They should have collected as much health data about the affected or deceased persons as it’s necessary to establish a possible causal connection, and a possible vaccine ingredient at fault.
They didn’t have this approach, which means they’re complete idiots. “The benefits outweigh the risks” can only be used in case of war, when even 1,000 collateral deaths are better than potentially millions of deaths, but so far no country has declared itself in a “state of war” with the COVID-19. Maybe they should have done so.
TWENTY-THREE
🟡 The “real thing” is that, if we are to believe what they say, the incidence of severe or life-threatening adverse reactions–in this case, thrombosis, blood coagulation issues, blood clots–aren’t higher than those normal in a population sample of the same age group and health condition. In plain words, this means that if you do the following…
- You vaccinate 1 million people with AstraZeneca’s jab and count the thrombotic reactions in the following 2 weeks.
- You give a free lottery ticket, a free newspaper issue, or a free Mars bar to 1 million people, just to have them in a list, then you count the thrombotic reactions in the following 2 weeks.
…you’re supposed to get similar results, with variations that are statistically irrelevant. If this is the case, this should have been properly explained to the population!
What EMA said in a press conference on March 16, one day after even Germany suspended AstraZeneca’s vaccine, wasn’t completely persuasive. Emer Cooke, executive director of the European Medicines Agency, said that through March 10, about 5 million AstraZeneca jabs have been administered, and only 30 suspicious cases have been reported. Suspicious, as in “thrombosis in patients without known blood problems,” I guess, because otherwise EMA knows of the following number of reports of adverse events:
- 102,100 for the Pfizer vaccine
- 54,571 for AstraZeneca
- 5,939 for Moderna
Once only the pathologies involving heart, vascular and blood problem are considered, the figures drop to:
- 17,056 for Pfizer
- 3,798 for AstraZeneca
- 1,099 for Moderna
In the case of AstraZeneca, it was the specific cases of thrombosis that triggered the decision for a precautionary stop in so many countries. But they still insist that only about 30 such cases out of 3,800 were “suspicious” (and severe)?! Also, how about the suspicious deaths, were they 2, 3, 5, or how many? We can’t trust the press, and we can’t trust the authorities either. Oh, wait, do they mean… 30 suspicious deaths?
We want precise and relevant numbers, and they’re not given to us. I’m quite sure AstraZeneca is safe, but the public won’t be persuaded neither through political reassurances nor by using a political ban on this vaccine!
At least, they’re not accusing the Russians or the Chinese of spreading fake news regarding this vaccine…
TWENTY-FOUR
🟡 A new episode in the current season of Idiocracy–The COVID-19 Edition. First, let’s say I’ve got some actual figures for the AstraZeneca-related “suspicious cases” in Germany, from Deutsche Welle’s AstraZeneca: What’s the deal with thrombosis? and Opinion: Do not write off the AstraZeneca vaccine:
- Cerebral venous sinus thrombosis (CVST) is the thing that worries everyone.
- Germany: 7 cases in 1.6 million people that got AZ’s jab (8 people if we count a later case).
- UK: 3 cases in more than 11 million people that got AZ’s jab (underreporting? different age groups?).
- For Germany, that means 4 cases in 1 million (5 cases if we consider the eighth one) for those vaccinated; compare to the natural occurrence in the general population, of 2…5 per million per year.
Now, the Germans apparently consider all the pros and cons: yes, the contraceptive pills give thrombosis in about 1,100 women per million, but no, it’s not the same type, as it’s a leg vein thrombosis, and it’s not as severe as this one. And yes, even if the incidence between vaccinated and non-vaccinated people is similar, the natural occurrence is measured per year, whereas here we have something that happened within about 6 weeks; still, the naturally occurring CVST usually happens in seasons of weather change, so the comparison might still be valid. But what they didn’t say is that the natural occurrence is determined for all age groups, whereas in Germany they have inoculated only the essential personnel and those over 80. So it’s not the same age distribution, which makes this vaccine still somewhat suspect.
What everyone should have said is this: only people who have platelet aggregation issues and don’t know it, or don’t treat the condition, might find this vaccine to behave as “the last drop” that triggers a potentially lethal cerebral venous sinus thrombosis. In plain terms: if you’re sick but you take your treatment, you should be fine. If you didn’t make a recent blood test, you’d better do it before getting the jab! (As a matter of fact, even in the much-lauded Germany, the family practitioners don’t insist that their patients make their annual checkup, and this is a huge idiocy; if I owned a health insurance company, I’d force all the insured people to make all the blood tests available twice a year, including all the cancer-related markers; this way, the insurer wouldn’t need to pay for expensive and potentially useless treatments of a disease that was discovered too late!)
But they’re not me, and I’m not them. They lack the most elementary logic; as for crisis management… no comment.
Let’s cheer up, though. EMA declared AstraZeneca’s jab safe on March 18; effective the next day, Italy, Germany, Spain, and other countries resumed vaccination. But Norway, Sweden and Denmark decided to wait, whereas Finland… just suspended it, citing two cases of post-vaccination blood clots! I left the best for the end: France decided to resume vaccination, but only for people over 55! Why? Their suspicious cases were under the age of 55! (Like I said, most likely people who weren’t aware of their blood issues.) But, were it indeed something wrong with the vaccine, wouldn’t older people being more at risk? (France was that country whose president initially said AstraZeneca’s jab is “useless” for people 65+, instead of saying that, given the lack of studies, it might be unsafe to such ages, but by no mean useless.) UPDATE: End-March, Germany suspended the use of AstraZeneca for under-60s. The Paul Ehrlich Institute has confirmed 31 cases of rare blood clots in recent recipients of the AstraZeneca vaccine, of which 29 were women aged 20 to 63; nine of them died. For the UK, there were still only 30 blood clot cases, with seven deaths, for 18 million doses.
One more episode of Idiocracy–The COVID-19 Edition. When on March 8, the German Bundesländer decided to open all the stores and barber shops wherever the 7-day incidence was under 50 (the target for normalization being under 35; different levels of restrictions imposed for the ranges 35-50, 50-100, 100-1000), non-essential stores reopened in my county (Landkreis Böblingen). But since March 18 they closed again, because on March 15 the 7-day incidence raised over 50!
In truth, most counties in Baden-Württemberg are having the 7-day infection rate between 50 and 100 (in 100,000 people), but in my opinion, this time the raise wasn’t caused by misbehavior and illegal parties, not even by schools. The testing has been intensified, many people from various services where human interaction is important having been tested up to twice a week; also, some idiots wanted to go to Mallorca (7-day incidence about 21) via Stuttgart Airport, so they went to be tested before that, and bingo, this way many people who didn’t know they were COVID-positive now got exposed! But this way the infection figures for most Landkreise went up, and so were the restrictions!
This is never going to end. I fucking want a Sputnik jab! Here, have some positive propaganda from Vox:
- Why you can’t compare Covid-19 vaccines (of course you can, but vaccines such as J&J’s have been tested more recently, on more virulent variants such as the South African one; should we retest Pfizer or Moderna’s jabs today, their effectiveness might prove diminished; but either way, all vaccines are 100% effective as long as you don’t get intubated and, more important, you don’t die!)
- Vaccine side effects are actually a good thing (at least some of them; my take is that people who experience unpleasant flu-like symptoms to a COVID-19 vaccine would have experienced similar initial symptoms to a COVID-19 infection, but without the vaccine, they risked death; those who had no side effect whatsoever might be of those who are asymptomatic even when they have the virus)
- Can we get rid of Covid-19 forever? (no; most likely it won’t be the case)
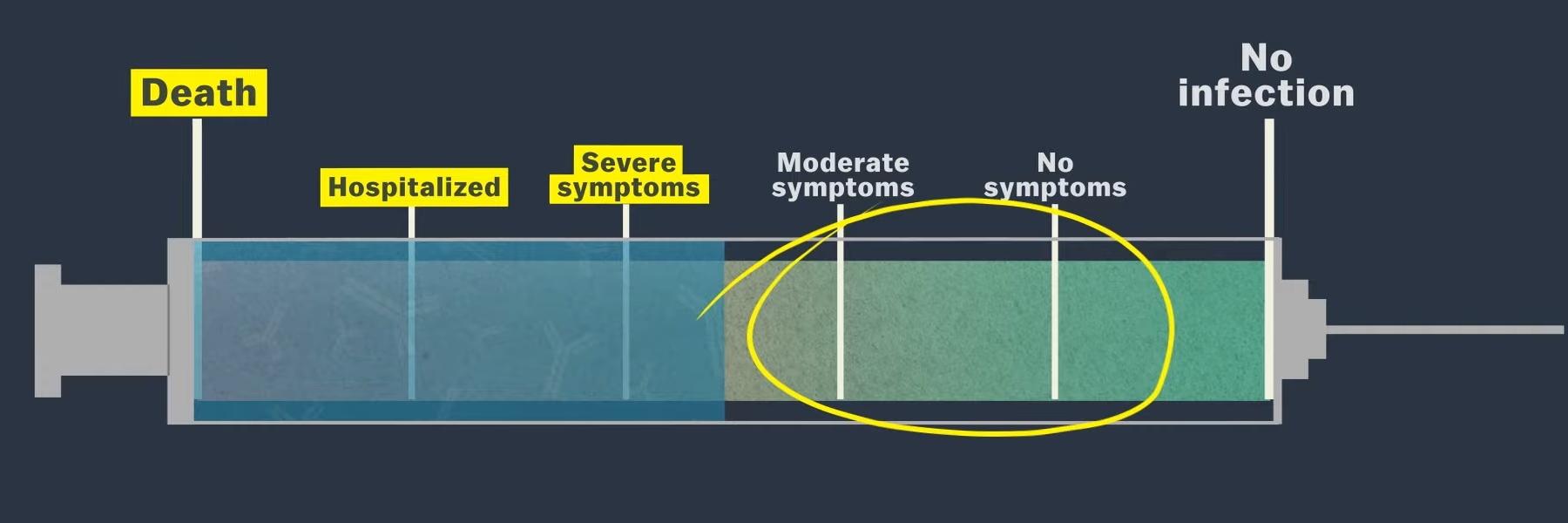
This being said, it’s not roses all the way: AstraZeneca to be exempt from coronavirus vaccine liability claims in most countries
AstraZeneca has been granted protection from future product liability claims related to its COVID-19 vaccine hopeful by most of the countries with which it has struck supply agreements, a senior executive told Reuters. …
“This is a unique situation where we as a company simply cannot take the risk if in … four years the vaccine is showing side effects,” Ruud Dobber, a member of Astra’s senior executive team, told Reuters.
“In the contracts we have in place, we are asking for indemnification. For most countries it is acceptable to take that risk on their shoulders because it is in their national interest,” he said, adding that Astra and regulators were making safety and tolerability a top priority.
Dobber would not name the countries. …
The United States, however, already has a law to exclude tort claims from products that help control a public-health crises in the form of the 2005 Public Readiness and Emergency Preparedness, or PREP Act.
TWENTY-FIVE
🟡 I’m starting to believe Germany is a criminal state. Both the Federal Government and the 16 Länder, with their 16 Ministerpräsidenten. They’re all stupidly criminal.
Exhibit A. Despite the increasing number of infections, the Kultusminister of the federal states have agreed to keep the schools open. In Germany, the Kultusministerium is that medieval institution in a State that’s Ministry of Education and of Cultural Affairs, but also (as the name literally means) of Religious Affairs (in some Länder). No air purifiers, no quick tests, no vaccinations for teachers, and yet, not jeopardizing the school year was more important to these politicians and bureaucrats than human lives. Reiner Haseloff, Ministerpräsident of Saxony-Anhalt, but also the current President of the Bundesrat, just explained how “we had to open schools and daycare centers and accept more infections, otherwise we would have had to write off the school year”. [What followed was a tweet that’s now deleted.]
The scandal is only in the social media; the mainstream newspapers have (all of them!) only commented on his accidental “covfefe” moment, the tweeting of a single “Ä”:
Yeah, this is Germany. Collective imbecility.
Exhibit B. For regions having a 7-day infection incidence in 100,000 people between 50 and 100, the German Federal Chancellor and the 16 Ministerpräsidenten have invented two concepts meant to pretend they allow some shops and businesses to remain nominally open, so that they can’t demand financial help from the State:
- Click&Collect
- Click&Meet
Yes, that’s in Denglish. Click&Collect means you order online or by phone, then you go to the respective brick-and-mortar store and pick your package at the front door. No, you cannot just show up at the door and say “I see your store is empty and you’re not busy, can you sell me this item at the front door?” Das ist verboten.
Click&Meet is even more pervert a concept. You need to make an appointment, online or by phone. Then, at the agreed time and for an agreed period, you can visit the store, after having left your personal data at the entry, in a register. The purpose is to limit the attendance to one person per 40 m² instead of the regular limit of one person per 20 m². The criminal thing here is that this concept doesn’t work, and it doesn’t make any sense either!
First, when such a store is practically void of customers, why can’t one just show up at the door and request entrance? Das ist verboten. But even with a prior appointment, one still has to stop and the entrance and write down their personal data in a register, so why can’t they just do that without any appointment, if the store is almost empty? Stupid bureaucrats. And yet, they just re-elected Winfried Kretschmann for the third time in Baden-Württemberg! He’s killing their businesses (not to mention he’s a Green and will kill the non-electrical cars), but they voted for him!
Secondly, Click&Meet, just as Click&Collect, just can’t work. One cannot make enough sales to justify the costs with so few possible customers! And how can they be scheduled? In time slots of 15 minutes? Of 20 minutes? What if they need more time because they really want to buy something? Or fewer time, when they can’t find anything to suit their needs? This is by no means a workable business model.
The vaccination rate is lame in Germany. They’re killing whatever wasn’t already dead in the local economy. They really are criminals and imbeciles.
TWENTY-SIX
🟡 No, I take it back. Above all, they’re shit stupid. Take this: Angela Merkel backtracks on Easter lockdown after uproar.
The “Easter mini-lockdown” was meant to fail, as it simply wasn’t well-thought-out. For instance, everyone should have stopped working on Thursday, April 1st. OK, but then what: were they supposed to be paid less, or from where should their employers have got the money to pay them, given that they weren’t working?
No problemo though. Local “hotspots” can take adequate measures, but even as Hamburg returned to a full lockdown, I can’t help but notice how that their mask-wearing rules in open spaces are different in different parts of the city; there are 54 areas and five kinds of timeframes:
- between 8 and 22 hours
- between 10 and 20 hours
- between 18 and 4 hours over the weekend (starting on Fridays)
- between 10 and 18 hours over the weekend (starting on Saturdays)
- between 8 and 15 hours on Saturdays
Please, tell me I’m dreaming. They don’t know shit, they don’t understand shit, yet they’re scrupulously devising stupid rules. They don’t have anything in their empty, bureaucratic heads, except for some worms, after they die.
TWENTY-SEVEN
🟡 Wave after wave, we exhibit more and more of our structural idiocy as a society, and as a species. Everyone only cares about going to Mallorca, to a Greek Island or wherever else they feel in vacation, but many countries or provinces who tempted a relaxation were forced to switch back to lockdown mode (from France to Ontario).
As long as most countries are grappling with the vaccination (the slowness of the vaccination in Germany is a shame and a huge failure of the entire Administration, local and Federal!), it’s clear that for most people, the only chance to get some protection is to catch the virus and to survive it!
But then, just as in 2020, too many deaths will occur because of people let to struggle with the disease at home, without proper treatment, for the lack of severe symptoms; when they finally go to the hospitals, it will be too late for some of them–watch The need for early management in patients with COVID-19 (slides in English, voice in French).
The problem is a purely bureaucratic one. The State and Pharma and Medical Mafia bureaucracy:
- doesn’t want people to self-medicate themselves, except with paracetamol and ibuprofen;
- doesn’t want to allow people to take drugs such as antibiotics and antivirals without medical supervision;
- doesn’t trust people, basically.
I know that some people are so dumb that they’d kill themselves even when only taking the most innocuous medicines, but the presumption of idiocy kills, as it forbids the dispensing of “COVID home treatment kits” (as suggested by some medical doctors, e.g. in Italy by the doctors in the #TerapiaDomiciliare group).
As long as outpatient (ambulatory) treatment is considered, the hydroxychloroquine administered early still proved its efficacy at Marseilles–Hydroxychloroquine en ambulatoire : 8400 patients COVID traités à l’IHU en 2020; Analyse critique des traitements de la COVID-19.
Another bureaucratic idiocy that kills: as long as thrombosis is feared, both in those infected and in those vaccinated with AstraZeneca, no fucking medical authority bothered to say that, excepted some specific contraindications, an aspirin a day won’t kill anyone, and it helps a lot! Watch Aspirine et COVID-19 (slides in English, voice in French); but maybe it has to do, for both aspirin and hydroxychloroquine, with the planned obsolescence of classic drugs.
Gallery not found.In the section numbered NINE, I mentioned Prof. Didier Raoult and “La piste du vison (the mink track)”; guess what? The powers that be still don’t care about that! Pourquoi cache-t-on la séquence des visons ?
We’re dumb. And doomed.
The new kid to the party? The Breton variant B.1.616 (aka 20C/H655Y), which might get undetected by the nasal swab tests (mouth probes are recommended).
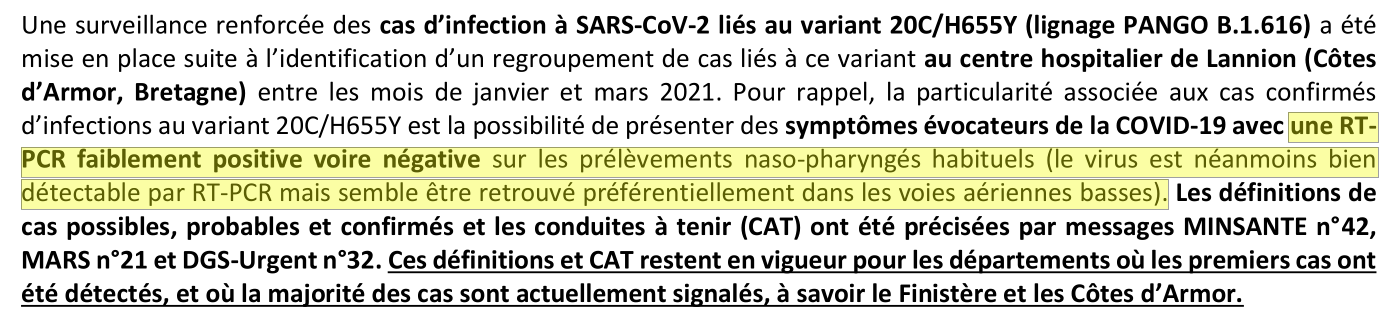
The Variants of Interest and the Variants of Concern are many more though; as per the CDC; and as per the French Santé Publique:
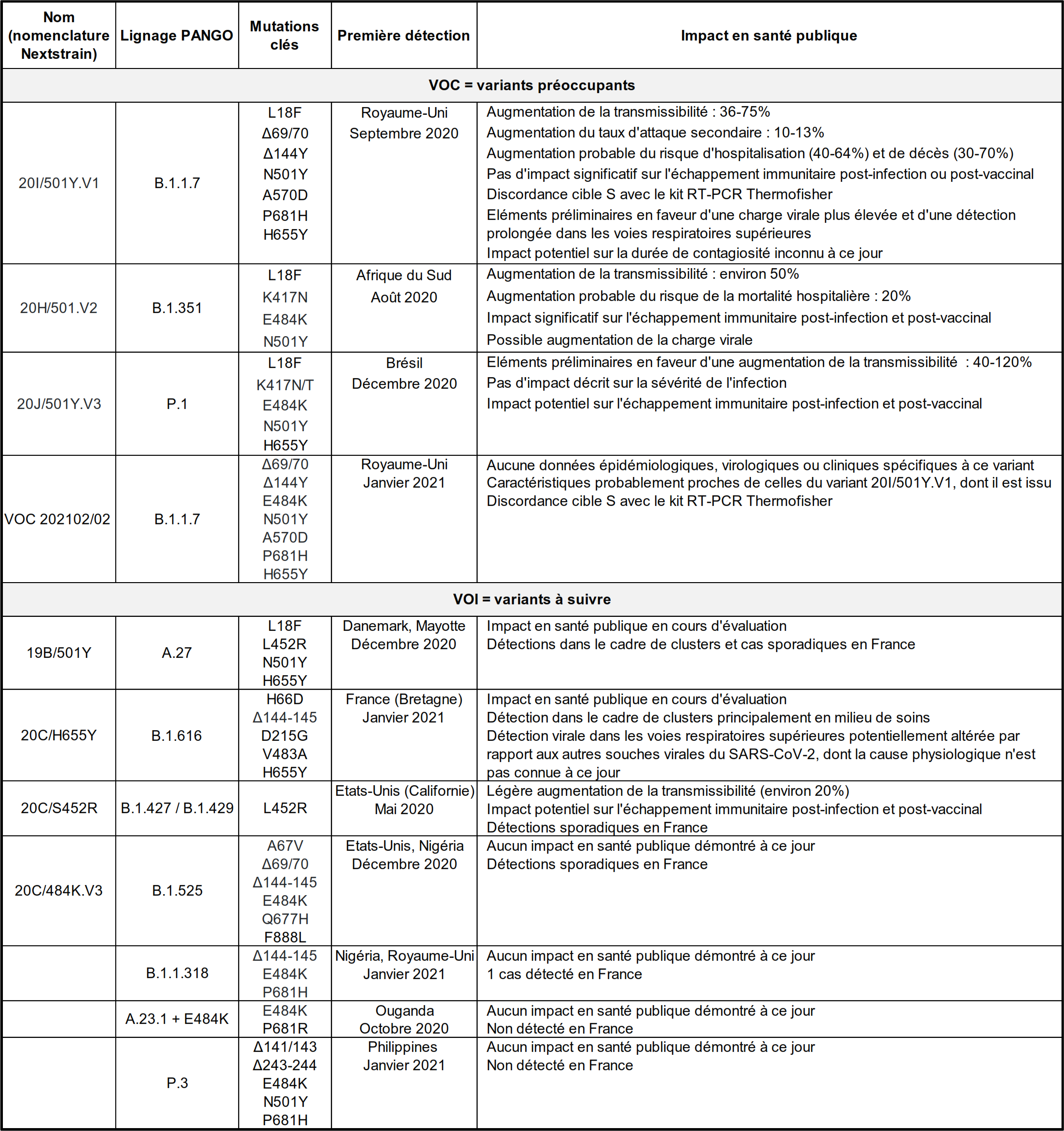
TWENTY-EIGHT
🟡 Stupidity, thy name is Ivermectin! A fad coming from the US, the dumb belief that Ivermectin, a drug used to treat parasite infestations (in humans: head lice, scabies, river blindness, strongyloidiasis, trichuriasis, ascariasis, and lymphatic filariasis; in veterinary medicine: heartworm and acariasis), and also used to treat acne rosacea and blepharitis when caused or exacerbated by Demodex folliculorum mites, might be the miracle drug against COVID-19, but the powers that be prefer to see us dead than to let us use it… well, this fad seems to have gained momentum in countries ranging from South Africa to Italy and Romania.
While I still believe that hydroxychloroquine can help a lot in the initial stages of the infection (if administered from the outset or preventatively, and in the same modest dosage as in preventing malaria), because there’s a known immunomodulatory mechanism of the (hydroxy)chloroquine that makes it useful e.g. in lupus, and a known anti-inflammatory mechanism that recommends it in rheumatoid arthritis, so I can’t trust FDA’s advice against HCQ, there is a lot of sense in FDA’s Why You Should Not Use Ivermectin to Treat or Prevent COVID-19.
SARS-CoV-2 is not a macroscopic parasite, full stop.
TWENTY-NINE
🟡 It was bound to happen. On April 14, Denmark became the first country in Europe to abandon AstraZeneca’s COVID vaccine completely. (“In Denmark, two recipients of the [about 150,000 people who received the] AstraZeneca vaccine have suffered severe blood clots, one of which was fatal.”) Two days later, according to a French minister, “The European Union is very unlikely to renew its Covid-19 vaccine contracts with pharmaceutical company AstraZeneca.”
The same day, and after 6 people out of 7.2M who received the Johnson & Johnson vaccine in the US developed blood clots, the CDC issued a Recommendation to Pause Use of Johnson & Johnson’s Janssen COVID-19 Vaccine.
We’re irremediably stupid as a society. We stopped vaccination for blood issues having an incidence of 5 per million for AZ and less than 1 in a million for J&J.
BTW, the reason some people get blood clots with AZ seems to be related to a protein called PF4 (Platelet Factor 4), according to a new study published in The New England Journal of Medicine: Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. Such people developed platelet-activating antibodies directed against PF4, causing a pro-thrombotic disorder strongly resembling heparin-induced thrombocytopenia, despite not having received any heparin. This is a form of vaccine-triggered autoimmune thrombocytopenia (AITP) which, unfortunately, doesn’t respond well to the usual treatments for thrombocytopenia.
🤔 This being said, j’ai l’impression que le Pr Didier Raoult ne s’est pas fait vacciner.
But the supreme proof of mass idiocy at the highest level could be seen in the infamous hearing of Dr. Fauci during a House of Representatives panel on the COVID-19 on April 15, when the shithead Rep. called Jim Jordan (R-Ohio) repeatedly yelled to Dr. Fauci, asking “When will the Americans get their First Amendment liberties back?”
Longer versions here and here.
Such politicians are worse than any pandemic.
THIRTY
🟡 Dr. Geert Vanden Bossche and the COVID-19 Apocalypse. That’s a new theory, saying that people should not get vaccinated, because the vaccine acts like an antibiotic, helping the virus to mutate in more dangerous variants!
This Belgian virus expert has a site dedicated to spreading his theory. His credentials:
Geert Vanden Bossche received his DVM from the University of Ghent, Belgium, and his PhD degree in Virology from the University of Hohenheim, Germany. He held adjunct faculty appointments at universities in Belgium and Germany. After his career in Academia, Geert joined several vaccine companies (GSK Biologicals, Novartis Vaccines, Solvay Biologicals) to serve various roles in vaccine R&D as well as in late vaccine development. Geert then moved on to join the Bill & Melinda Gates Foundation’s Global Health Discovery team in Seattle (USA) as Senior Program Officer; he then worked with the Global Alliance for Vaccines and Immunization (GAVI) in Geneva as Senior Ebola Program Manager. At GAVI he tracked efforts to develop an Ebola vaccine. He also represented GAVI in fora with other partners, including WHO, to review progress on the fight against Ebola and to build plans for global pandemic preparedness. Back in 2015, Geert scrutinized and questioned the safety of the Ebola vaccine that was used in ring vaccination trials conducted by WHO in Guinea. His critical scientific analysis and report on the data published by WHO in the Lancet in 2015 was sent to all international health and regulatory authorities involved in the Ebola vaccination program. After working for GAVI, Geert joined the German Center for Infection Research in Cologne as Head of the Vaccine Development Office. He is at present primarily serving as a Biotech/ Vaccine consultant while also conducting his own research on Natural Killer cell-based vaccines.
His theory:
Why do Covid-19 mass vaccination campaigns promote dominance of selective immune escape variants?
“Mass vaccination campaigns can substantially reduce infection rates and hence, the emergence of new viral variants. So, enhancement of vaccination campaigns should be able to prevent circulation of additional variants.” Why is this simplistic postulate fundamentally wrong? First, in order for emerging more infectious variants to enhance their potency and become well established, they must adapt to the suboptimal immune pressure they escaped from. To adapt viruses to grow at high infectious titers under suboptimal conditions, it is critical to passage the virus repeatedly under the same ‘stress’ conditions. Likewise, repeated person-to-person transmission of a highly mutable virus under similarly selective, suboptimal immune pressure would enable ‘training’ of selected immune escape variants. This will ultimately result in adaptation of the viral variant and thereby enable full-fledged replication under conditions which initially restricted its replication. All more infectious Sars-CoV-2 variants are characterized by mutations that are directed at spike (S) protein (herein called: ‘S variants’). Selection of S-directed mutations enables enhanced binding of these variants to the ACE-2 cell receptor. By virtue of their enhanced binding to cell receptors on respiratory epithelial cells, S variants are able to overcome limitations in infectiousness imposed by S-specific antibodies (Abs).
In the absence of infection prevention measures or mass vaccination campaigns, spontaneously occurring S variants have no opportunity to compete with circulating wild virus as there is no selective immune pressure mechanism promoting their adaptation to the human host. In case of de novo infection of a seronegative population with Sars-CoV-2, there is no selective immune pressure that could promote replication and propagation of immune escape S variants. In case subjects have previously been primed as a result of infection with wild type Sars-CoV-2, their later exposure to variant S antigen (S’) will recall a strong response mounted by Abs that effectively recognize both S and S’ (https://science.sciencemag.org/content/early/2021/03/24/science.abg9175). Lastly, subjects who are in the process of seroconverting as a result of Coronavirus (CoV) infection will not be susceptible to re-infection by another CoV due to antiviral innate immunity. So, in none of the above-mentioned cases do S variants have an opportunity to repeatedly replicate and propagate under suboptimal selective immune pressure. This is to say that under conditions of natural infection, adaptation of S-selective immune escape variants does not usually occur. This seems to be confirmed by the results from virus characterization on archival autopsy samples from subjects who succumbed to Influenza during the pandemic of 1918. Samples isolated during the second, most severe, wave did not indicate any contribution from variant strains (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3291398/).
In case of mass vaccination, however, there is plenty of opportunity for spontaneously occurring S variants to experience selective immune pressure. Mass vaccination campaigns will cause large, not previously primed cohorts of the population to seroconvert against S protein and to even maintain suboptimal Abs for quite some time (e.g., in those waiting for the second dose of a 2-shot vaccine) while being exposed to spontaneously emerging viral variants. Such cohorts include people who have not previously been infected at all as well as subjects who have been asymptomatically infected and only exhibited short-lived Ab titers, presumably due to lack of adequate priming (https://www.medrxiv.org/content/10.1101/2020.12.18.20248447v1; https://www.nature.com/articles/s41392-021-00525-3). Mass vaccination of vulnerable groups does not abrupt viral transmission chains but increasingly redirects transmission events to asymptomatic carriers (i.e., vaccinated subjects as well as not yet vaccinated young and healthy people, several of whom experienced asymptomatic infection without mounting long-lived Ab titers). As ongoing mass vaccination campaigns are shifting the ‘reservoir’ of viral transmission to asymptomatically infected subjects (whether vaccinated or not), the likelihood for unvaccinated, previously asymptomatically infected subjects to experience re-infection with Sars-CoV-2 while being endowed with suboptimal and short-lived ant-S Abs substantially increases. This is to say that within the population that is now most actively involved in viral transmission, new, spontaneously emerging S variants have plenty of opportunities to train under suboptimal immune pressure such as to ultimately adapt to the human host and become part of the dominant circulating Sars-Cov-2 population. This is how – after initial breeding of selected viral variants as a direct result of infection prevention measures – subsequent mass vaccination campaigns will drive enhanced circulation of additional, more infectious viral S variants. ‘Training’ of such more infectious immune escape variants is thought to be reflected by the plateau that follows the vaccine-mediated decline in cases and the height of which exceeds the one following the previous wave of cases.
As mass vaccination campaigns have started in the vulnerable population, not only vaccinated subjects but also not yet vaccinated younger age groups will become a breeding ground for new infectious variants. There can be no doubt that continued mass vaccinaton campaigns will enable new, more infectious viral variants to become increasingly dominant and ultimately result in a dramatic incline in new cases despite enhanced vaccine coverage rates. There can be no doubt either that this situation will soon lead to complete resistance of circulating variants to the current vaccines. This is certainly not what would be expected by those who claim that enhanced and accelerated mass vaccinaton is going to diminish circulation of new dominant variants and will, therefore, further reduce viral infection rates and flatten morbidity and mortality curves.
Author: Geert Vanden Bossche, DVM, PhD (March 31 2021) – www.geertvandenbossche.org
😡 First of all, this guy is an idiot; but before elaborating on that, let’s say that he includes: supportive references from the literature; supportive references (quotes and documents); and critical unresolved questions.
Some of his “critical questions” are actually going against his theory and against logic. Say:
How to explain the sudden emergence of several, more infectious variants (e.g., UK, South-African, Brazilian variants) in QIV 2020 (i.e., prior to the roll-out of mass vaccination campaigns and despite relatively low infection rates)?
Well, dear genius virologist, mutations occur even without vaccination, and “sudden” is not a scientific term. Biological rhythms are different between species.
How to explain the increase in cases of severe Covid-19 disease in younger (< 60 years), previously protected, age groups as currently observed in several countries?
It’s very simple: they weren’t “protected”! Also, just as with every single respiratory infection (the common cold is given by a coronavirus) people of all ages were spreading it, and even more so the kids! The claim so dear to some epidemiologists and virologists, all as smart as a dead dog, that “there are no studies to confirm that kids are spreading SARS-CoV-2” is as logical as the claim “there’s no study to confirm that this brand of carbonated water is wet, because we only have studies for other brands of carbonated water”!
🧑🔬 Now, to get to some common sense:
- Yes, the so-called “immune evasion” exists. But it happens regardless of vaccination or non-vaccination. Variants resistant to what someone’s (or some group’s) immune system “learned” to fight against appear all the time. It’s how viruses work! (Of course, my comparison with antibiotics is not correct: an antibiotic only fights bacteria and has typically no effect on viruses, although incompletely explained exceptions exist; and antibiotic-resistant bacteria appear because that antibiotic was used and for no other reason.)
- Yes, sometimes this “immune evasion” is increased by mass vaccination, but you know why? Because the mass vaccination at a level that doesn’t eradicate the epidemic or pandemic helps more people to escape death, thus allowing the “evading” resistant virus strain to further spread to many more people! The alternative would be to accept more deaths.
- No, nobody said that when mass vaccination occurs, but the “herd immunity” is not reached and the pandemic is still there, vaccinated people should stop taking the established preventive measures! (Gestes barrières in French.) The proof that it was understood that a vaccine primarily protects its recipient resides in the fact that most countries still require negative tests from vaccinated people who come or return from abroad!
It’s as simple as that. Stopping the mass vaccination would be a criminal act.
Here’s a scientific article, if you don’t trust my judgment, from the Office for Science and Society of the McGill University, Montréal: The Doomsday Prophecy of Dr. Geert Vanden Bossche. A Belgian virus expert has scared the Internet by claiming the COVID-19 vaccines will doom humanity. No need to panic.
This is not complete nonsense. I reached out to Dr. Paul Offit, a paediatrician specialized in vaccines and immunology and the co-inventor of the rotavirus vaccine, to get his thoughts on whether antibiotic resistance and vaccine-associated immune escape are indeed comparable. “In a sense it is, but he misses the main point,” Dr. Offit told me. A vaccine shows your body an inert part of the virus so that it can make neutralizing antibodies against it. If the body ends up making low levels of these antibodies, i.e. not enough to swiftly kill the virus when you catch it, this could allow the virus to stick around in your body for a little bit and make copies of itself. Some of these copies may by chance have the right kinds of errors in their genetic code to become variants of concern, although the mutation rate of this coronavirus is quite low.
“But if you have a vaccine that results in high levels of neutralizing antibodies, that’s not a way to create variants,” he continued. To use an analogy, if a gaggle of invaders is coming but you have only managed to round up a few soldiers, be prepared for a long siege during which the enemy might learn a thing or two about your defences and adapt. But if you have a full and overpowering army at your command, the invaders won’t stick around for long. So the question becomes: do the COVID-19 vaccines give us low or high levels of neutralizing antibodies?
…
But even if the COVID-19 vaccines were “leaky,” meaning they still allowed some vaccinated people to transmit the virus to others, there is evidence that they could still efficiently contain the spread of the disease. Edward Nirenberg, a science blogger who addressed Dr. Bossche’s claims in great detail, points to Marek’s disease. It is caused by a herpes virus and it gives chickens a number of health problems, including cancer. Thankfully, there is a vaccine against it, but over time, newer and more virulent strains of the virus have been detected, and this made scientists think it was because the vaccine was leaky, that it did not allow the chicken to mount a good enough immune response. Interestingly enough, the use of this seemingly leaky vaccine in chickens led to a reduction in the incidence of Marek’s disease by 99%. Potentially leaky vaccine but stellar disease reduction.
Another important counterpoint to Dr. Bossche’s claim is that we can simply reformulate our vaccines to match new variants of concern. There is a reason why a new flu vaccine is made each year: the influenza virus drifts and shifts and the vaccine needs to be reformulated to be a better match for the specific viruses that are predicted to be common during the next flu season. Similarly, if a new SARS-CoV-2 variant emerges and is so different that our current crop of vaccines don’t match it, scientists can simply tweak their vaccines. It’s not an instantaneous solution, as massive vaccination campaigns require manufacturing and deployment at scale, but it’s a fix we know well and have implemented in the past.
…
If Dr. Bossche fears the current vaccines so much, what is his solution?
…
Our immune system is divided into two main branches: innate and adaptive. … Vaccines make use of the adaptive part of our immune system.
Dr. Bossche, however, seems to be a big fan of the innate immune system and he worries that all of these COVID-19 vaccines and public health measures are getting in the way of our innate immune system fighting off the coronavirus. He claims that keeping people in lockdown during the pandemic is not beneficial to their innate immune system, which requires exposure to viruses and bacteria to remain in tip-top shape. This is a bad argument. As Dr. Offit pointed out to me, even at home we are exposed to legions of microorganisms. “The food you eat isn’t sterile,” he reminded me, “the dust you inhale isn’t sterile, the water you drink isn’t sterile.” We get exposed to a lot of microorganisms.
This innate immunity gambit on the part of Dr. Bossche is something typically seen in wellness communities obsessed with the naturalistic fallacy, where strengthening your immune system is as simple and as natural as taking in the sun, walking in the woods, and hugging people. For Dr. Bossche, however, the solution is not long walks on the beach, but an alleged new type of vaccine focused on training the innate immune system. One of the cell types of the innate immune system is a natural killer cell, and Dr. Bossche claims to be developing a natural killer cell vaccine. Have we seen any evidence of this? No. I believe I speak for many scientists when I say: show us the evidence.
Imagine you were a public health advisor and were confronted with this choice: to heed Dr. Bossche’s apocalyptic warning and stop all COVID-19 vaccinations (scenario #1) or to ignore him and follow the evidence (scenario #2). What would you do?
…
Dr. Geert Vanden Bossche is a veterinary doctor who also has a Ph.D. in virology. His LinkedIn profile lists several jobs in upper management positions, including a three-year stint as the senior program officer for vaccine discovery at the Bill and Melinda Gates Foundation. He is no stranger to vaccines. His academic publications essentially stop in 1995, except for one 2017 article about his natural killer cell vaccine idea published in a journal belonging to a publishing group, OMICS Group Inc, that has been called “predatory” and was sued by the Federal Trade Commission for deceptive practices.
When you read Dr. Bossche’s open letter, you should pick up on the Galileo gambit, which is when you infer that because Galileo was laughed at but ultimately correct, your laughable idea must also be correct. You should pick up on his apocalyptic language (“there is no time to spare”, “if we are committed to perpetuating our species”) and turns of phrases that would be more at home in a superhero movie (“guardians of mankind”). You should pick up on the tactic too often used by anti-vaccination promoters: “I am all but an antivaxxer.” You should subsequently pick up on the types of people who grab this manifesto and endorse it for their audience, people like Robert F. Kennedy, Jr and Del Bigtree, known figureheads of the modern anti-vaccination movement.
…
In short, if we are concerned about the virus mutating to evade vaccine protection, the solution is to vaccinate as many people as quickly as possible and to eventually reformulate the vaccines to match variants of concern that acquire this ability. And if we are concerned about the anti-vaccination movement, we should wonder why they were so quick to prop up the portentous letter of an alleged pro-vaccine scientist.
McGill’s article ends with a “take home” summary I won’t copy here. My “take home” message is different:
- Dr. Bossche is an idiot. He’s not a complete fraud, despite being a veterinarian. (Funny thing, his PhD degree in Virology from the University of Hohenheim, Germany, is not in his LinkedIn profile, but I suppose it’s real.)
- Dr. Bossche being such an idiot who doesn’t understand how a vaccine works, whoever hired him in his previous positions that were vaccine-related (GSK/GlaxoSmithKline Biologicals 1998-2006, Novartis Vaccines & Diagnostics 2006-2007, Solvay Biologicals 2007-2008, Bill & Melinda Gates Foundation 2008-2011, Global Alliance for Vaccines and Immunisation 2015-2016) should be fired for not having noticed how idiot he was.
- Vaccines don’t increase the “natural” innate capacity of the immune system to fight pathogens; they increase the adaptability of the immune system, by teaching it how to fight new patterns prior to having encountered such patterns in nature, to prevent deaths occurring from having met such pathogens while having an “uneducated” immune system. Whoever claims the contrary shouldn’t be allowed to work in health-related fields!
The “natural” way an immune system works is like this: a body encounters a pathogen (virus or bacteria); subsequently, the body does or does not develop medical symptoms (in the case of most pathogens we encounter we don’t get sick), while it learns how to develop antibodies to fight the said pathogen; in case there are symptoms and a medical condition develops, the body must remain alive and its fight with the pathogen must be successful to make sense of having learned to develop such antibodies! As there are pathogens that kill a smaller or a larger part of those infected, and as there are also pathogens that let people crippled for life (polio, anyone?), vaccines were invented to help minimize the casualties.
A so-called virologist doesn’t understand that, and he is trying to kill more people than Stalin, Mao and Pol Pot together. Don’t let him do it! 🥺
THIRTY-ONE
🟡 New proofs of a pandemic of mass idiocy. While a new “double mutant” SARS-CoV-2 strain named B.1.617 is rapidly spreading in India, idiots all over the globe fuel a new wave of fake news and conspiracy theories.
Some such refurbished theories, and a few new ones include:
- Facemasks are ineffective in slowing down the spreading of the virus, and they “can cause hypoxia, hypercarbia, health deterioration, and premature death,” therefore “mask mandates are a crime against humanity.” Funny thing, those who know what asthma is (myself included) didn’t die as of yet. Also, surgeons never complained about the requirement to use surgical masks. Last but not least, the Asian (primarily Japanese) habit of wearing face masks when the city pollution is too high seems to contradict the hypoxia-cum-hypercarbia theory.
- THOUSANDS OF PEOPLE DIED AFTER HAVING BEEN VACCINATED AGAINST COVID-19! No comment.
- This virus DOESN’T EVEN EXIST! “This is pseudoscience, and we’re in a tyranny without any evidence of a virus!” Of course, they forgot to complain that quarks, bosons, and leptons can’t be shown to the public, therefore they don’t exist.
- “Vaccines are provoking miscarriages, but not only to vaccinated women; even women who have had contact with vaccinated women are having miscarriages. THE VACCINE IS THE VIRUS!” Tales of miscarriages and or painful periods are relayed by the likes of Daily Mail, and by social networks for retards, such as Reddit, for some months already. But the many retarded inhabitants of Planet Earth (“in our image, in our likeness“) are oblivious of the fact that women are more likely to experience hormonal adverse reactions TO ALL TYPES OF VACCINES, including the flu shot! There’s absolutely nothing new and nothing specific to the COVID-19 vaccines!
What’s new is the fact that this pandemic has increased the level of mass idiocy on Planet Earth, population 7.860 billion. Let’s hope for the swift death of many of the most retarded, while being sorry for the unnecessary death of the others.
THIRTY-TWO
🟡 FUD stands for Fear, Uncertainty, and Doubt. And this is what even some well-intentioned people do these days. Take the European Media Director of Human Rights Watch, who expressed his view in a long thread (20+ tweets) that starts here:
Read the whole thread by opening the tweet in a new window. Only after you’ve done that, read below.
💉This guy here starts a thread (READ IT!) that mixes truths&idiocy.
NO, the scarcity isn’t artificial.
YES, with only 2.8% vaccinated, we’ll never make it.
NO, it’s not an issue of patents, as Resolution 58.5 of the World Health Assembly already includes a TRIP Waiver clause! https://t.co/YFLGEauNTd— Ludditus ex-Béranger (@ludditus) April 24, 2021
For the soft-headed:
Apparently, too many people don’t understand the difference between a patent waiver and a TRIPS waiver: TRIPS waiver: Pressure mounts on WTO as supporting voices grow. The patent waiver possibility IS INCLUDED IN TRIPS AND IN Resolution 58.5 of WHA, so there’s no need for a TRIPS waiver! The situation has been detailed more than two months ago in an Italian newspaper (look under “Sospensione del monopolio”).
Is this planet only populated by morons?
THIRTY-THREE
🟡 As of end-April 2021, COVID-19 is still a hoax to some. The virus either doesn’t exist, or it doesn’t kill much. It either cannot be transmitted through air, or it can, but face masks are totally useless. Demonstrations against COVID-related measures take place regularly in Europe.
On the other hand, relaxation measures are considered, or already taking place in a number of countries. A 50,000-person concert in New Zealand (without masks), because, you know, last month Spain hosted a 5,000-person indoor concert (with masks and tests) and it went well (it was for lesbians, and maybe they’re immune). The CDC relaxed the rules for vaccinated people.
What’s the right thing to do? I don’t know, but what I know is that a relaxed approach is responsible for the current situation in India that could lead to millions of deaths. Enjoy your freedoms and liberties!
THIRTY-FOUR
🟡 The patent saga vs India. I talked about patents in chapters NINETEEN and THIRTY-TWO, and I linked to an Italian article from Feb. 8, to Art. 31 of TRIPS, and to Resolution 58.5 of the World Health Assembly. Anyone and everyone could see that in such an emergency, patents can be waived by unilateral decisions of national governments. You don’t have to be a lawyer to understand that.
This planet full of retards whined and moaned, petitioned and cried “you bloody rapacious bastards, set the vaccine patents free!” First of all, if a country such as India wants to declare a nationalization of the US patents for Pfizer’s and Moderna’s vaccines, they are free to do it under the aforementioned regulations. They only have to notify the WTO and the US. But such vaccines are extremely difficult to produce, and India currently has huge difficulties even in something as simple as TRANSPORTING SOME BLOODY OXYGEN CYLINDERS across the country (Il Post; BBC), so given their structural and fundamental flaws, how could they possibly produce and transport mRNA vaccines that need storage at -70°C or -20°C? True enough, the Serum Institute of India has manufactured AstraZeneca’s vaccine under the name Covishield, and a national one called Covaxin, but they’re both traditional vaccines. And India shouldn’t complain that they don’t have enough vaccines as long as they’re still exporting them by millions!
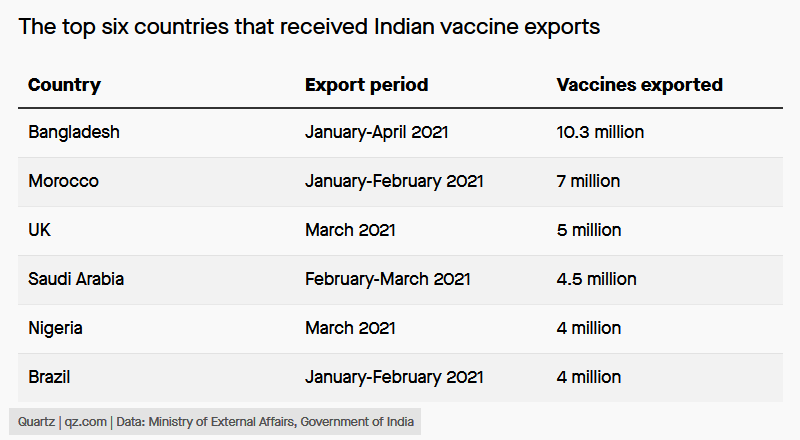
But here’s the so-called “big news”: U.S. backs waiving patent protections for Covid vaccines, citing global health crisis. Except that, in their understanding,
the WTO’s discussions over waivers could take time and, since the body’s rulings are based on consensus, will require approval from all 164 members.
No kidding. What consensus? Why should it take time? TRIPS dixit:
Article 31
Other Use Without Authorization of the Right Holder
Where the law of a Member allows for other use of the subject matter of a patent without the
authorization of the right holder, including use by the government or third parties authorized by the
government, the following provisions shall be respected:
(a) authorization of such use shall be considered on its individual merits;
(b) such use may only be permitted if, prior to such use, the proposed user has made efforts to obtain authorization from the right holder on reasonable commercial terms and conditions and that such efforts have not been successful within a reasonable period of time. This requirement may be waived by a Member in the case of a national emergency or other circumstances of extreme urgency or in cases of public non-commercial use. In situations of national emergency or other circumstances of extreme urgency, the right holder shall, nevertheless, be notified as soon as reasonably practicable. In the case of public non-commercial use, where the government or contractor, without making a patent search, knows or has demonstrable grounds to know that a valid patent is or will be used by or for the government, the right holder shall be informed promptly;
Then, WHA 58.1, initially adopted for a tsunami, but applying to all similar emergencies:
URGES Member States:
…
(10) to take all necessary measures during a global pandemic, to provide timely and adequate supplies of vaccines and antiviral drugs, using to the full the flexibilities contained in the Agreement on Trade-Related Aspects of Intellectual Property Rights;
It can’t be any clearer than that, but not for this nincompoop:
This is a monumental moment in the fight against #COVID19. The commitment by @POTUS Joe Biden & @USTradeRep @AmbassadorTai to support the waiver of IP protections on vaccines is a powerful example of 🇺🇸 leadership to address global health challenges. pic.twitter.com/3iBt3jfdEr
— Tedros Adhanom Ghebreyesus (@DrTedros) May 5, 2021
Once again, India’s problem with vaccines isn’t the patents issue. They can manufacture as many of AstraZeneca’s as they want! But can they do more? It’s not like the former GDR said: “Look, in our Trabant factories (factories, plural, because parts have to be made too) we’d have happily made your Mercedes, if it weren’t for the patents!” Let’s get real.
This doesn’t mean I’m all in for patents; on the contrary, I’m against all kinds of patents, because:
- A patent is an immoral monopoly that extends over a too long period of time.
- Most patents are trivial and don’t reward “hard work and huge investments” etc. Some simply patent “business ideas”!
- Many “inventions” occur in the normal engineering work, so any patent that’s granted practically forces many people and companies to look for alternate solutions, just because their genuine work happens to have found a technical solution that’s been patented by someone else. Even in Marconi’s time, an invention could have been “discovered” almost simultaneously by several people unaware of each other. Any such patent legitimizes one inventor’s theft of other people’s work, because the others cannot use their genuine work!
- With hundreds of millions of patents, any engineering company has fewer costs with the actual engineering and designing than it has with digging in the patents databases to see whether their solution doesn’t happen to infringe some patents and, as in most cases it does, to re-engineer their products to avoid legal issues! This isn’t only immoral, that’s unbelievably stupid!
- I am sure that millions and millions of patent infringements are undiscovered, because there aren’t enough people on Earth to check all the technical implementations against all the valid patents!
- This is even more valid for software patents, most of the time disguised as “device and apparatus that etc. etc.” followed by a few charts describing the general idea of an algorithm; software means algorithms, and algorithms shouldn’t be patentable. Anything that every single software developer is doing every single day is probably infringing some fucking patent, but who can check on that, even if all software were open-source?
- Patent trolls are the lowest form of moral abjection.
- In the end, patents hinder the development of the society, despite the theory stating otherwise.
The world needs a revolution on patents, I’ll grant you that. But this isn’t going to happen right now.
This doesn’t change the fact that BioNTech’s CEO, Uğur Şahin, is an asshole:
Recently, Biontech’s boss Ugur Sahin also did not consider a waiver of intellectual property rights to be the right way to increase the production of Covid-19 vaccines. “This is not a solution,” he said. Biontech relies on close collaborations with select partners, he said, because its vaccine is difficult to manufacture. “There are opportunities we are considering that we give special licenses to competent manufacturers.” That would ensure the quality of the vaccine, he said. Production by licensees, however, could happen toward the end of the year at the earliest.
Further reading on the patent issue:
- Bulletin of the World Health Organization Volume 91, Number 7, July 2013, 465-544: Using TRIPS flexibilities to facilitate access to medicines
- Pope Francis is supporting universal access to the COVID-19 vaccine and a temporary suspension of intellectual property rights
- Angela Merkel Pushes Back on Vaccine Patent Waiver in Row With U.S.:
German Chancellor Angela Merkel weighed in against a U.S. proposal to waive patent protections for Covid-19 vaccines, casting doubt on whether the idea has enough international support to become a reality.
The U.S. plan would create “severe complications” for the production of vaccines, a German government spokeswoman said Thursday in an email. Without the incentive of profits from research and development spending, drugmakers might not move as aggressively to make vaccines in the future, the industry has argued.
“The limiting factor for the production of vaccines are manufacturing capacities and high quality standards, not the patents,” the German government spokeswoman said. “The protection of intellectual property is a source of innovation and this has to remain so in the future.”
She’s correct on the true limiting factor, but otherwise she’s an asshole.
And again: India cannot complain that they don’t have enough COVID vaccines as long as they exported 43% of what they produced, thus making about 85% of the COVAX program!
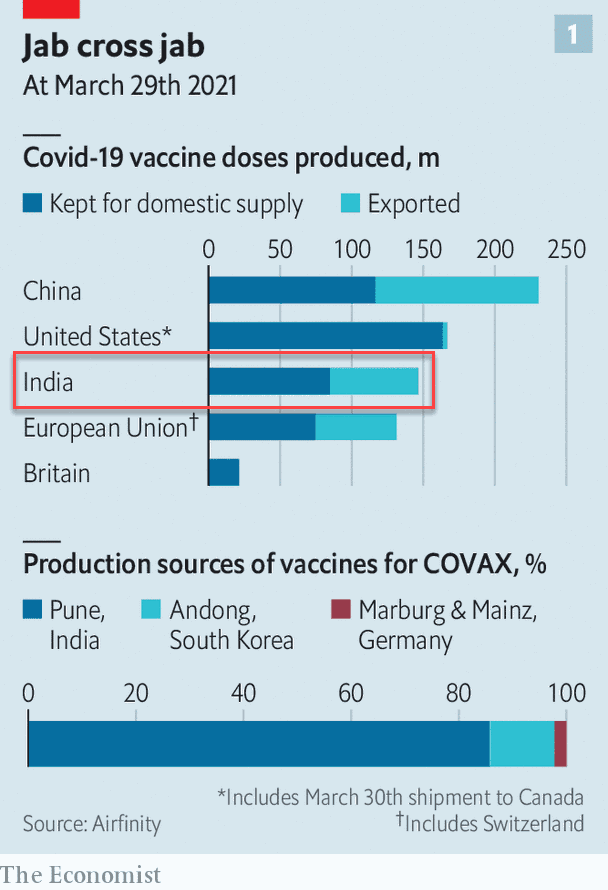
THIRTY-FIVE
🟡 Back to India, the situation seems dire, but how severe it really is? Let’s put things in perspective: absolute numbers can impress, but India has almost 1.4 billion people, so it’s to be expected. How about judging by new cases per 100k inhabitants?
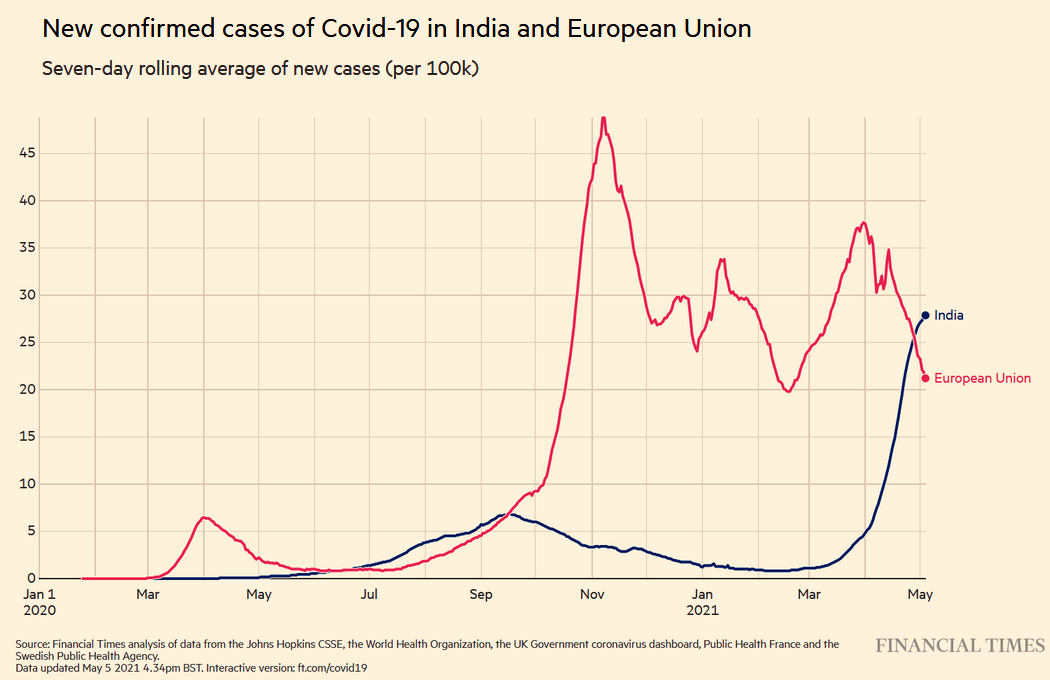
Wow. It has been much worse in Europe, wasn’t it?
Now, of course, with the abysmal level of misery and backwardness that’s endemic to India, we can expect a huge mortality. Look how they struggle to provide oxygen. As for actual treatments… you must be kidding, right?
Things surely can’t be improved when people who used to be quite smart are openly asking on social networks for new conspiracy theories:
Abjection at its best. COVID-19 revealed what’s worst in Homo sapiens sapiens.
THIRTY-SIX
🟡 I forgot about Sputnik’s mishaps! This wasn’t any good, was it? End-April: Brazil health regulator rejects Russia’s Sputnik vaccine … citing safety concerns. A very technical explanation by Dr. Angela Rasmussen, in this Twitter thread:
The Sputnik V vaccine Ad5 vector is evidently replication competent. The makers apparently neglected to delete E1, so getting this vaccine means being infected with live adenovirus 5. Hence Brazil’s regulator correctly rejected it.
Adenovirus-vectored vaccines like J&J, AstraZeneca, and Sputnik V use infection with adenoviruses, common pathogens that usually cause common colds. But to increase safety and decrease risk of side effects, most vaccine vectors delete the AdV E1 and E3 genes.
E1/E3 deletions are standard in Ad-vectors. Deleting E1 prevents the virus from replicating and deleting E3 prevents it from interacting with the immune system.
This results in a vaccine vector that causes a transient infection, due to the vector’s inability to complete its replication cycle. When I got J&J it infected my cells, began expressing viral proteins, including SARS-CoV-2 spike, and then hit a block because of the E1 deletion.
Sputnik V is a heterologous Ad-vectored vaccine: the prime dose is an Ad26-vectored vaccine (like J&J), followed by a booster that uses Ad5. This was apparently found in testing the Ad5 booster but I can’t emphasize how sloppy this is.
When making adenovirus-vectored vaccines, once you’ve deleted a region of the genome, it doesn’t just reappear out of nowhere. The presence of replicating virus suggests E1 was either not deleted or it recombined during manufacturing with a full length AdV genome.
And while strong statements from Gamaleya and the RDIF dispute the findings, this isn’t the first observation that the Sputnik V doses submitted to regulators aren’t consistent with the phase 3 trial results published in Lancet.
Slovakia’s drug regulator previously rejected a batch of Sputnik V for being substantively different than the batches reported in Lancet. The EMA has also said they have insufficient safety and QC data to authorize it in the EU.
This is disappointing. Ad-vectored vaccines are easier than mRNA vaccines to store and distribute, and are going to be important for vaccinating people in hard-to-reach places. Despite rare side effects, they are generally considered safe and trial data shows they are effective.
Safety concerns have already reduced enthusiasm for these vaccines, and an unforced error like this further amplifies those concerns and decreases trust in the technology itself. I hope Gamaleya resolves these issues and supports it with data and robust QC/QA.
Apparently the Ad5 vector was capable of forming plaques on A549 cells. The explanation is recombination, which begs the question: if it was manufactured using best practices, WTF did the vaccine vector recombine with?
Could be either a wild-type AdV or a packaging vector. To make replication-deficient vaccine vectors, you have to grow the virus in a “packaging” cell line expressing E1 in trans (on a separate piece of DNA called a plasmid).
At this stage recombination could occur with E1 DNA from the packaging cell line, but usually there are QC measures in place to ensure this doesn’t happen. Deleting E1/E3 in many Ad-vectored systems is also needed to make “room” in the genome for the insert, SARS-CoV-2, spike.
I don’t know enough about the specific AdV system used here, but it’s reasonable to think that if E1 recombined w/ the Ad vector, it might replace spike. So that’s doubly bad: you not only have a replication-competent Ad5, it’s not expressing spike. Which is … the entire point.
One thing is clear: if the vaccine were forming plaques on A549s, that means there’s infectious, fully replication competent virus there. A plaque is a “hole” in a carpet (monolayer) of cells on a culture plate caused by cytopathic effect (virus killing cells).
The plaque assay is a classical virological technique used to titrate infectious virus. An individual cell killed by a virus can’t be seen without a microscope. To see a plaque with the naked eye, the virus has to spread to surrounding cells, and to do that it has to replicate.
No visible plaque=no spread to surrounding cells=no viral replication. So if they saw plaques on A549s (a type of lung cell that is convenient for plaquing adenoviruses), that means there was fully replication competent virus.
It’s a basic and inexcusable failure of QC/QA.
Disappointing indeed. Not necessarily much more disappointing than what the “developed Western countries” are doing: how about Denmark totally dropping Johnson and Johnson’s vaccine “over side effects fears,” despite never having used it? Oh, the Danish Health Authority considered that “the benefits do not outweigh the risk”!
THIRTY-SEVEN
🟡 On curfews, again. You see, I’m constantly bothered that the effectiveness of face masks, of physical (“social”) distancing, and of other preventative measures has been questioned over and over again, and people protested that they don’t want to be “muzzled,” yet the curfews have barely been addressed. How’s that so?
Il Post had a nice feature, How effective is the curfew? It includes links to external articles and studies in English, but you should first use an automated translation of the article first. I’ll only highlight a few ideas:
• The most critical argue instead that they are useless if not counterproductive, because they reduce the time available for shopping or other activities after work, leading to a greater concentration of people in stores and therefore increasing the risk of contagion.
• Excluding the possibility of leaving one’s home at night, except for special needs, it is assumed that social interactions are reduced: the obligation to go home at 10 pm, in fact, is mostly a disincentive (or a logistical obstacle) to meet in a group the evening. Intended, it would also serve to limit activities related to alcohol consumption in the company, which can lead to less responsible behavior and to ignore good practices to reduce the risk of contagion. However, if the premises are still closed, or it is allowed to be found only in their open spaces, it is not clear how a curfew can help reduce particular risk behaviors.
• In the scenario in which the premises cannot absolutely accommodate customers in the evening, as happened in most of Italy until Sunday, a curfew could prove counterproductive by encouraging small groups of people to be at home, with the risks deriving from spending the time together indoors. The possibilities of control by the authorities during a curfew are also reduced, compared to those that could lead by controlling the premises that may be open even late in the evening.
• In these months of curfew it was also discussed whether the timetable applied in Italy made sense or if it was necessary to change it, according to some by shortening it and according to others by extending it. In France, for example, the curfew has long been in effect from 6pm to 6am, with severe restrictions on businesses. However, it is not clear whether a longer duration than that adopted in other countries has led to greater benefits. Especially in the early stages, the curfew meant that there were more customers lining up in front of the shops because the opening hours were reduced, with a consequent risk of crowding indoors.
• A preliminary study conducted in Luxembourg reported that a curfew from 11 pm would have a limited impact on the spread of the infection, but the researchers admitted that they could not take into account the behavior of individuals, linked for example, the choice to anticipate their social activities or purchases in stores.
• Another research, conducted by analyzing the restrictions imposed in about fifty countries, concluded that curfews together with lockdowns work in principle, but that it is not possible to evaluate the two measures separately since they are almost always adopted together. Another preliminary study has instead concluded that the curfew has moderate effects in containing the infections.
• With a curfew in effect since mid-October 2020 in most of its territories, France should offer numerous ideas, but even in this case the data does not seem to help much. A group of researchers from Toulouse attributed the decline in infections in the city to the curfew initially established at 8pm, but also noted a worsening of the situation when it was decided to trigger the limitations at 6pm in a second phase. Their hypothesis also in this case is that more people have started going to supermarkets and other shops at the same times, having less time available to shop.
• A study also conducted in France, and awaiting review, has identified benefits in the curfew to slow the spread of the coronavirus in some areas of the country in early January. However, the researchers report that the benefits seem to have diminished in the following weeks, when the so-called “English variant” (B.1.1.7), more contagious and difficult to contain, began to spread.
My opinion is that curfews are more like the enhanced security checks on airports after 9/11: they produce a lot of discomfort to law-abiding citizens, while doing close to nothing to prevent criminal acts.
WE, THE IDIOTS, are wearing masks.
WE, THE IDIOTS, are practicing distancing.
WE, THE IDIOTS, are not meeting people not living under the same roof with us.
WE, THE IDIOTS, are disinfecting everything.
WE, THE IDIOTS, cannot stroll a bit in the evening if there’s a curfew in place.
WE, THE IDIOTS, cannot go buy a book in a bookstore, because it’s closed.
THEY, THE CRIMINALS, are organizing illegal indoor parties, at no matter what time of the day or of the night.
THEY, THE CRIMINALS, are meeting with whomever they want.
THEY, THE CRIMINALS, are spreading the disease, but WE, THE IDIOTS, are to pay fines if we’re caught outside, in the fresh air, at curfew times!
So yeah, curfews are the most antidemocratic measure and the most useless one in the entire pandemic!
Also, could someone explain how people are free to go to Mallorca, with airports and aircraft bearing a huge risk of infection (not counting the stupid COBUS airport buses, always packed!), and how supermarkets don’t pose an important risk, but bookstores, department stores, and outside eating and drinking can’t be allowed?
We’re now really more stupid than in the Middle Ages, when judges were summoning pigs, and people burned “demonic” cats & “witches” and whatever nonsense were they doing back then. And there’s no hope for improvement: Idiocracy is our future!
Ugh. Upped to TWENTY sections, yet nobody cares, 20 days since I posted this.
I Care.
De fapt sunt impresionat.
TWENTY-TWO, with an update at the end of NINETEEN.
TWENTY-FIVE, when I really made my mind: they’re criminally stupid, even in Germany.
TWENTY-SIX. They don’t have anything in their empty, bureaucratic heads, except for some worms, after they die.
Thoroughness should be your middle name. Saved to Pocket to read it later.
Chapter TWENTY-SEVEN added.
TWENTY-EIGHT: Stupidity, thy name is Ivermectin!
TWENTY-NINE: AZ, J&J and Rep. Jim Jordan.
THIRTY: Common sense and McGill University against the Doomsday COVID-19 Prophecy of Dr. Geert Vanden Bossche.
THIRTY-ONE: New and refurbished conspiracy theories.
THIRTY-TWO: Fear, Uncertainty, and Doubt, from the European Media Director of Human Rights Watch.
THIRTY-THREE: A relaxed approach is responsible for the current situation in India that could lead to millions of deaths.
THIRTY-FOUR: The patent saga vs India.
THIRTY-FIVE: India again.
THIRTY-SIX: I forgot about Sputnik’s mishaps!
THIRTY-SEVEN: On curfews, idiots, and criminals.